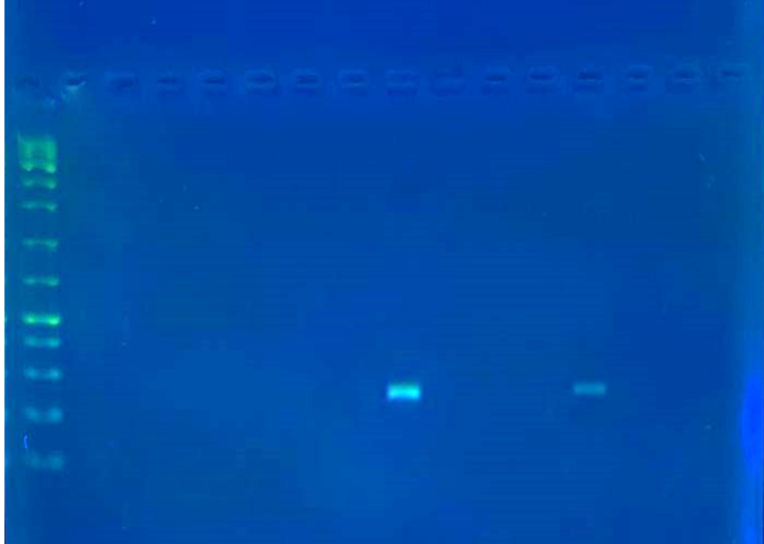
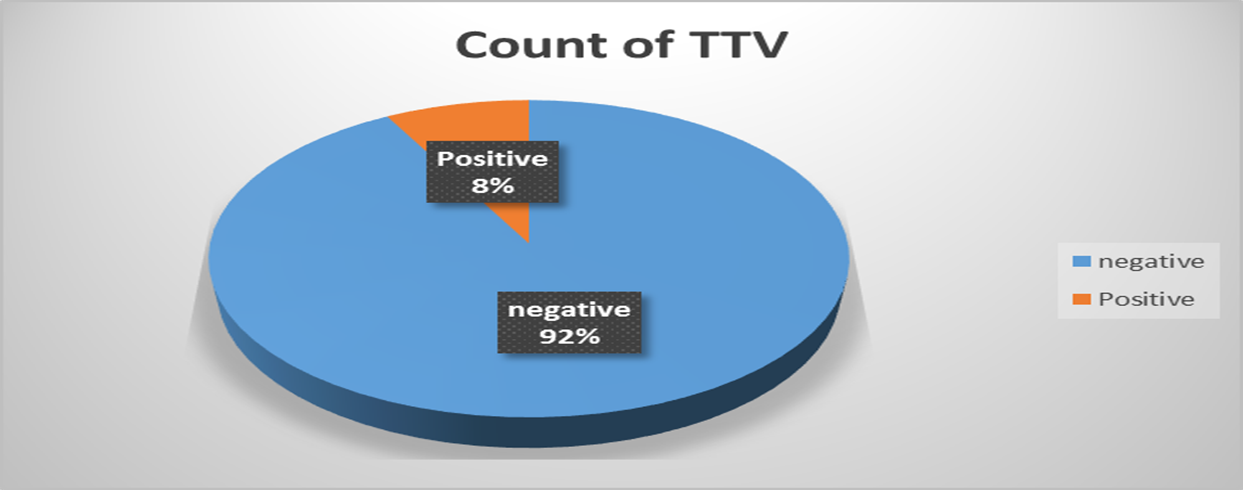
According to the nested polymerase chain reaction results, the infection rate of TTV was 8% depending on urine samples taken from women with urinary tract infections based on microscopic examination and cultivation who were admitted to Al-Batool Teaching Hospital for Maternity and Children. Women's Emergency Unit and Urological Consultation Unit at Baqubah Teaching Hospital in Diyala Governorate.
Neighbouring countries showed high rates of TTV infection compared to the current study, such as 21% in hemodialysis patients and 26.8% in β- thalassemia patients in Iran (22), 42.9% among hemodialysis patients compared with (19%) for the control group in Saudi Arabia (23). The rate in this study is relatively high compared to other studies, such as the Iranian study, which detected the virus in 4% of healthy individuals and 5.8% in HCV-positive persons (24).
The variation in TTV infection rates in different studies may be due to several factors, such as detection methods. Hence, the current study used a nested PCR technique. While others used quantitative polymerase chain reaction (qPCR). The qPCR method helped detect the most prevalent human TTV genotypes due to no cross-reaction with other viruses (25).
The second cause that may affect TTV infection rates is sample size and type of study population. In the current study, the sample size was (100) urine samples. While the study done by (26) used (607) blood samples and reported (55.4%) co-infected TTV/TTMV in a healthy population, to (96.3%) of TTV / TTMV coinfections of an HBV group in different nationalities by nested PCR in Qatar. Urine samples should be analysed within a short time (less than 1.5–2 hours) after sample collection due to high contamination risk because of multiplying bacteria. Moreover, it is challenging to store due to chemical preservatives resulting in changes in the pH and specific gravity (27). Changes in the environmental pH can induce morphological changes in empty proteinaceous shells occurring in viral capsids after DNA encapsidation (28).
The third cause is using multiple genes in different regions in the genome to detect TTV infection. Using N22 region detected (11%) and re-analyzed TTV prevalence with UTR region found TTV DNA was detected in(95%) of samples in eastern Taiwan indigenes (29). The detection of 5’-UTR primer results showed more prevalence of TTV DNA than N22 primer in patients and healthy control (30). Interestingly, the genome's conserved regions are non-coding areas (UTRs) in TTV and GC rich region, a poly-A sequence downstream and a TATA box and upstream are coding regions (31).
Other factors which may affect the result include immune status, nutrition, therapies, genetic makeup, geographical distribution, seasonal considerations, lifestyle choices (smoking, alcohol consumption, physical activity), and zoonotic transmission (32).
The results of the present study showed that most TTV infections were in the age group (31–46 years) at the rate of 75% (6 cases) while 1case (12.5%) in the age groups (17–30 years) and (63–77 years) with high statistical significance. These results agreed with a study that found TTV prevalence was significantly higher in the very young and elderly by using stool samples from people exhibiting signs of enteritis (954) and from non-diarrheic individuals (76), suggesting that immunological status is essential in infection by using qPCR assay in Canada (33).
A study investigating the association of TTV load and age found a slightly positive correlation with age within a cohort of (379) Italian elderly subjects (34), TTV load was significantly higher in the elderly (50–60 years old) compared to the young group (p < 0.001) during the investigation of TTV DNA load in plasma of (313) healthy persons using real-time PCR in Austria (35).
These results indicate that positive infection with TTV occurred in all age groups due to TTV infecting nearly all people indefinitely without the disease, establishing an acceptable and successful interaction with the host (36).
The current study showed a moderate rate of bacterial growth in relation to positive patient to TTV, who were diagnosed by using many biochemical tests (37), such as Staphylococcus aureus 3(37.5%) sample followed by 2(25%) samples for each of Escherichia coli and Proteus mirabilis. Finally, Enterococcus fecalis 1(12.5%) sample. This result agreed with the result of a study that found that (57.1%) of culture-positive and 100% of culture-negative samples demonstrated TTV DNA's presence, compared to none in the controls in Washington (38). The current study disagreed with a study that concluded that TTV is present in the vagina in many women with typical pregnancy outcomes and that its occurrence is associated with a lack of L. crispatus dominance, an increase in vaginal MMP-8 and a decrease in D-lactic acid in Brazil (39). Potent bactericidal activity was exerted by a minimal number of resident L. gasseri and L. crispatus strains showing the specific ability to produce and release antibiotic-like compounds. It eradicated the microbial pathogens pre-associated with the surface of cervix epithelial cells, providing efficient protection of the cells against the deleterious effects triggered by toxin-producing G. vaginalis and uropathogenic E. coli (40). The vaginal microbiota is a dynamic and often critical factor in this pathogenic interplay because changes in the vaginal microbiota characteristics result in the loss of ordinarily protective Lactobacillus spp., thus increasing the risk of UTI. These alterations may result from the influence of estrogen deficiency, antimicrobial therapy, contraceptives, or other causes (41). The variation in bacterial growth in the study population could be related to the fact that most UTI women have taken antibiotics for treatment.
According to the available information, the present study is considered the first study in Diyala Governorate to deal with a phylogenetic analysis of TTV. The PCR product's sequencing revealed eight local isolates. After nucleotides sequencing and amino acids analysis, a significant alignment with Torque Teno Virus strain NA-MU 15 ORF1 gene, partial with accession number (ID: KY750543.1) length: 269 were produced by using NCBI and MEGA 6 software. The sequences analysis results showed many mutations (transition and transversion) at TTV genome-related by ORF1-N22 region except the local isolate (No. 3) that was 100% identical with the reference isolate Torque Teno Virus strain NA-MU 15 ORF1 gene. All eight isolates nucleotides sequence analysis showed high identity with this reference isolate ranging between 98–100%. Also, high identification ranged between 96–100% with amino acids sequence analysis of all local isolates with this reference isolate.
According to the closest in the phylogenetic tree, the variation between local isolates and reference isolates ranged from 0.01 to 0.03. Distance 0.01 between (isolate No. 6 and reference isolate from Egypt and isolate from the USA), (No.3 and No.7) and (No. 2 and No.5). Distance 0.02 between isolates (No. 6 with reference isolates England, Australia and Saudi Arabia). Also, local isolates (No. 1 and No. 6) and (between local isolates No.4 with No.8). Distance 0.03 (between local isolate No.1 and Italian and Brazilian isolates).
The local isolates may have had multiple recombination and mutation in the Iraqi population this cause the generation of a large number of TTV variants driven by the high mutation rate, which is closer to RNA virus (42). Regarding the phylogenetic tree analysis of eight local isolates, there is a high diversity among them, the phylogenetic tree constructed by the neighbour-joining method according to (43) using MEGA 6 and NCBI software, showed that local isolates clustered with the Egyptian isolate revealed by (44) which reported TTV in a high prevalence among children with thalassemia and non-thalassemic individuals with genotypes 1 and 2. Isolate No. 6 was close to the Egyptian isolate ID: KY750543.1, American isolate ID: AF397741.1, England isolate ID: AF146809.1, Australian isolates ID: AF212332.1 and Saudi Arabian isolate ID: AY256672.1. Local isolate (No. 1) clustered with Italian isolate ID: AJ402241.1and Brazilian isolate ID: DQ665287.1, while local isolates (No.3) showed close relation to isolate (No. 7), isolate (No.2) and isolate (No.5) are very closely related and isolate (No.4) clustered with isolate (No.8) and all these six isolates were close to the Iranian isolate with the accession number ID: GQ179967.1 as shown in Figure (2). This study agreed with the study done by (45) who found that phylogenetic analysis indicated that the most common genotype of TTV among Saudi Arabia is 2. Furthermore, the study found that the data indicates that TTV is widespread genotypes 1, 2 and 3 in Italy in parenterally exposed subjects and that the infection frequently persists (46).
The current study with (17) also disagreed with a Brazilian study which found that the prevalence of TTV in healthy individuals was 69.0% by using ORF N22 primers (47). These results can be explained by the rapprochement between the two countries, sharing water resources, trade exchange and religious tourism, and travelling for study and treatment. Many factors cause high variation in the TTV genome, even in the same geographical area. Amplification of ORF1 (N22 region) gives high diversity among strains when used in phylogenetic analysis (48).
The cause of widely distributed TTV infection among human populations might be explained by multiple transmission modes (9). This could be related to increased travel and communication to a different area for learning, treatment and tourism. Moreover, TTV can transmit by multiple routes such as spreading by exhalation (49) and particles of TTV shed into faeces, demonstrated that they might be highly resistant to the water environment (50).
{kind=link}
{kind=link}