As we were unable to collect data at Time 2, we present here baseline and Time 1 results only.
Recruitment
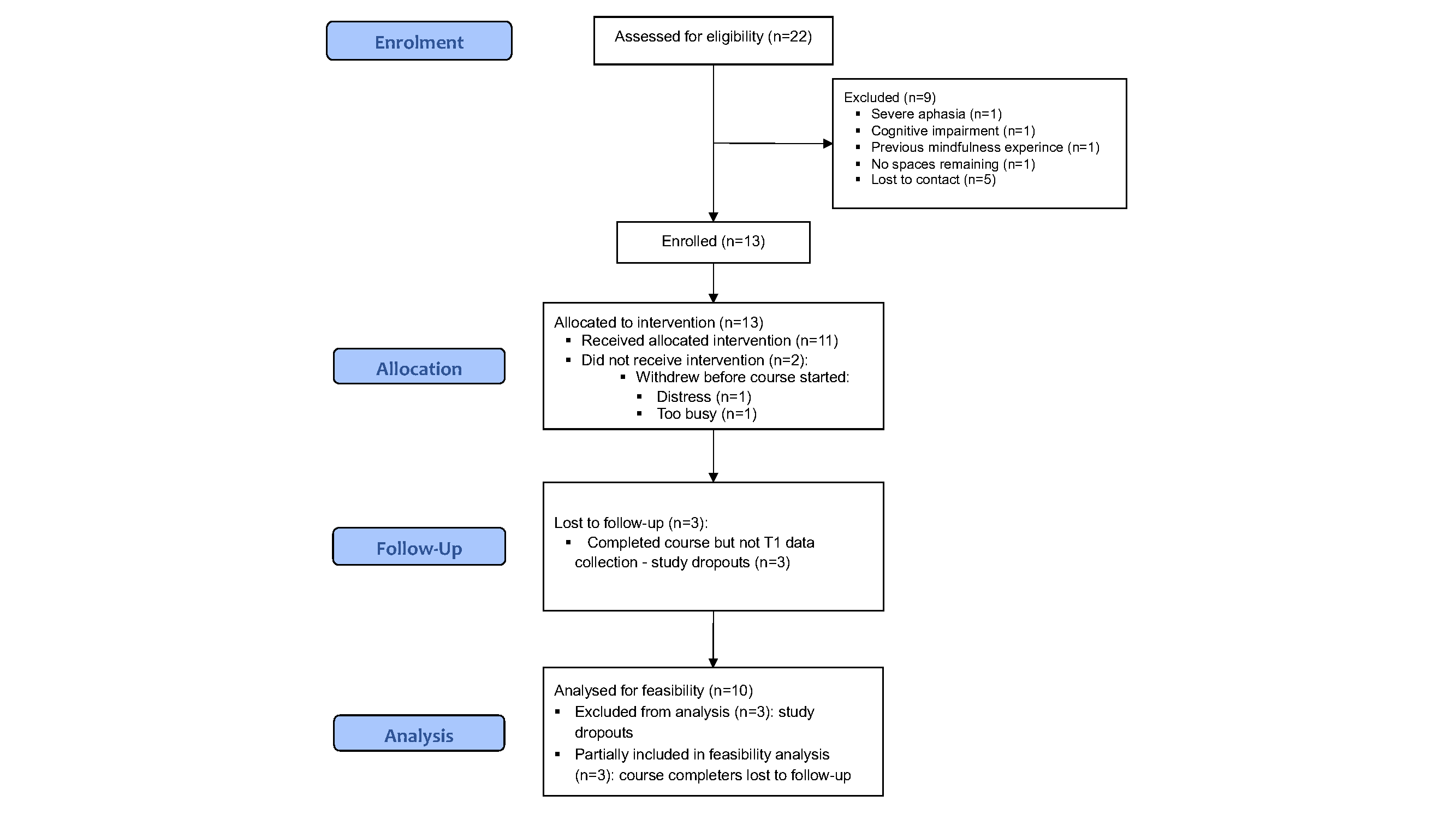
We recruited over 9 weeks (August to October 2019). Thirty-one individuals expressed an interest; 22 were assessed for eligibility; 13 (59.1%; female n = 4, 30.8%) were enrolled (1.44 per week). Nine stroke survivors (40.9%) were excluded during screening (lost to contact n = 5, 55.6%; severe aphasia n = 1, 11.1%; severe cognitive impairment n = 1, 11.1%; previous MBSR experience n = 1, 11.1%; recruitment closed n = 1, 11.1%), see Diagram 1 CONSORT flow diagram. We actioned SOP 1 (high HADS scores) for 12 (92%) stroke survivors.
Five stroke survivors nominated a family member to take part with them (female n = 4, 80%; spouse n = 4, 80%; peer n = 1, 20%). Stroke survivors were aged 63.3 (SD 10), male n = 9 (60%), 28 (IQR 34) months post-stroke, and educated to college level (or higher) n = 10 (76.9%). Family members were aged 67.7 (SD 9.2), male n = 1 (20%), and educated to college level (or higher) n = 2 (40%); all participants were Caucasian (see Table 1).
Table 1
Participant characteristics - Studies 1 and 2
| |
Study 1
(n = 13)
|
Study 2
(n = 9)
|
| |
N
|
%
|
N
|
%
|
|
Age Median (IQR)
|
66 (14)
|
58 (12)
|
|
Gender
|
|
Male
|
9
|
69.2
|
4
|
44.4
|
|
Female
|
4
|
30.8
|
5
|
55.6
|
|
Time Post-Stroke (months)
|
|
Median (IQR)
|
28 (34)
|
23 (10–38)
|
|
Living Arrangements
|
|
With spouse/family
|
11
|
84.6
|
9
|
100
|
|
Alone
|
2
|
15.4
|
0
|
0.0
|
|
Ethnicity
|
|
White Scottish
|
10
|
76.9
|
4
|
44.4
|
|
White Other British
|
2
|
15.4
|
3
|
33.3
|
|
White Non-Specific
|
1
|
7.7
|
2
|
22.2
|
|
Employment Status
|
|
Retired
|
8
|
61.5
|
3
|
33.3
|
|
Part-Time Employed
|
1
|
7.7
|
2
|
22.2
|
|
Full-Time Employed
|
2
|
15.4
|
0
|
0.0
|
|
Unemployed
|
0
|
0.0
|
2
|
22.2
|
|
Part-Time Volunteer
|
0
|
0.0
|
1
|
11.1
|
|
Long-Term Sick
|
2
|
15.4
|
1
|
11.1
|
|
Highest Educational Attainment
|
|
Completed Secondary
|
3
|
23.1
|
1
|
11.1
|
|
College or above
|
10
|
76.9
|
8
|
88.9
|
|
HADS mean (SD)
|
|
TOTAL
|
18.62 (4.9)
|
22.4 (6.7)
|
|
HADS-A
|
10.08 (2.9)
|
11.4 (3.0)
|
|
HADS-D
|
8.54 (4.3)
|
11.0 (4.4)
|
|
Legend
HADS: Hospital Anxiety and Depression Scale; IQR: Interquartile range; SD: Standard deviation
|
Completion of outcomes
Mean change in outcomes scores across the scales were positive and in the expected direction for both stroke survivors and family members (see Additional file 3). Data reporting completion of PROMs is presented in Table 2.
Table 2
Completion of PROMS - Studies 1 and 2
|
Completion of PROMs
|
Study 1
|
Study 2
|
| |
Stroke survivors (n = 13)
|
Family members
(n = 5)
|
Stroke survivors
(n = 9)
|
|
Baseline
|
At least partial completion of all PROMs
|
10 (76.9%)
|
3 (60%)
|
5 (55.6%)
|
|
At least partial completion of ≥ 1 PROM
|
0 (0%)
|
1 (20%)
|
0 (0%)
|
|
No completed PROMS
|
3 (23.1%)
|
1 (20%)
|
4 (44.4%)
|
|
Time 1
|
At least partial completion of all PROMs
|
6 (46.2%)
|
3 (60%)
|
5 (55.6%)
|
|
At least partial completion of ≥ 1 PROM
|
1 (7.7%
|
0 (0%)
|
0 (0%)
|
|
No completed PROMS
|
6 (46.2%)
|
2 (40%)
|
n = 4 (44.4%)
|
|
Legend
PROMS: Patient Reported Outcomes Measures
|
Feasibility and acceptability of research processes
Screening
Participants understood the importance and relevance of eligibility screening and described the process as ‘well thought out’. However, completing the MoCA/BADS was burdensome
[the MoCA & BADS were] quite demanding ... mentally, it got a bit tiring, particularly towards the end of it … I did OK, but it really taxed me (SS10, Int2)
Completion of questionnaires
Participants often described an altruistic motivation for completing the questionnaires, but the number of questionnaires was overwhelming
It does wear you [out] you know ... maybe it is a little bit too much, but I don’t know, I haven’t went through it all yet, I have done about 3 pages … (SS10, Int2)
One participant described their reluctance to report accurately the help they needed; another pointed out that for people with physical disabilities, completing paper forms was challenging. They welcomed a suggestion to make the questionnaires available online.
Feasibility and acceptability of the HEADS: UP intervention
Course preparation
Participants had received pre-course illustrated information sheets that gave them an idea of what to expect from the course. Not ‘coming in cold’ was an important factor in alleviating anxiety about embarking on something new and unfamiliar
The [accessible information sheets] were absolutely fabulous! I have never been given such clear instructions … (SS3, FG2)
In week 1 participants attended an introductory session ahead of the core course (weeks 2–9). This also proved helpful in reducing any anxiety about taking part in a group and the actual course:
[the introductory session] was quite useful because it did give us a chance to meet each other and hear the stories … [it] was a good way into what mindfulness was about because not everybody maybe knew about it (SS2, FG2)
Learning mindfulness techniques
Most participants found learning the various breathing meditations particularly helpful in controlling feelings of anxiety, as they were available to them whenever they needed them, irrespective of their immediate environment
I think the breathing for me is really, really good … it works for me as well. Sometimes situations happen, and as I say especially with the breathing, you can do it any time and it works (SS6, FG1)
For some participants other mindfulness techniques proved challenging. For example, several people found the body scan required some time to master, but once achieved, this could be used in the same versatile way as meditations of the breath:
I just couldn’t really get into it and I just I thought it was a waste of time to be honest ... what’s the point? Well, I find myself noo [now] on the bus doing it! I realise I am actually doing it and yet I didn’t like it [laughter] (SS7, FG2)
Personal practice: Participants received paper copies of weekly session material from the HEADS: UP manual along with audio recordings of the mindful practices they had been taught. Participants engaged well with these resources, making frequent use of them. As with other practices they found them versatile and ‘portable’, drawing on them when and wherever they recognised rising symptoms of anxiety:
I find the voice files very, very helpful. I used it while I was sitting in the hospital with my wife, trying to comfort her. But it also helped me to reduce [my] anxiety (SS3, FG2)
Participants understood the importance of personal practice, essential to master the skills taught during the course and in general found the supportive materials helpful:
It’s not a quick fix and you have got to persevere at it … it is practice, practice, practice and you have got to be prepared to do it or it is a waste of time coming (SS6, FG1)
Finding the time and motivation to practice was often challenging, especially for participants who experienced fatigue, or found that busy lives intruded:
There doesn’t seem to be a great time then for me. It is either ‘I have got to walk the dog’ or ‘I have got to do this’, ‘I have got to shop’ or whatever. I don’t know. I found it difficult to fit it into the day and then in the night I am generally far too tired, and I fall asleep even if I mean to do it. So I found that a bit tricky you know, to find a good time to do it (SS11, FG1)
However, participants understood the importance of persevering with their mindfulness practice and incorporating it into everyday life, but many were unsure about how they could do this, once the course ended:
I am not sure how I will take it forward although I want to … (SS3, FG1)
Groupwork
Participants found being part of a group with common experiences and goals beneficial, growing in their mindfulness experience together
it was good that I was learning new skills, I was listening to other participants and getting feedback … it is the first time I have ever been in a group with people that ... [are in] a similar position [have had a stroke] (SS7, FG2)
Dyads
Participants who attended in dyadic partnerships found working with a family member beneficial as their post-session discussions reinforced their learning from the weekly sessions and meant they could experience mindful moments together outwith the course. One participant, who had decided to attend alone, described belatedly understanding the benefit of attending with a family member having observed others’ interactions
The fact that you have come [as a couple], and you can both hear it [mindfulness] fresh, and you know how to deal with it, … I think it probably works better than coming here on your own … and I can’t believe I have just said that! (SS3, FG1)
Personal impacts
Participants described being ‘at the beginning’ of a long journey but reported perceived benefits including stress reduction, ‘living in the moment’, and improved relationships
I think I am a different person … I don’t [get angry with] my husband as much now, so I think he is quite happy [laughter in the group]. I am a much calmer person … (SS3, FG1)
Optimisation
Optimisation of the intervention and research processes was undertaken following completion of data analysis. However, imposition of Covid-19 restrictions which had resulted in early termination of Study 1 also necessitated changes to the design of the programme of work. Consequently, we decided to adapt the optimised, in-person intervention and research processes for online delivery and to test these in a subsequent non-randomised feasibility study (Study 2). Table 3 presents an overview of the optimisation and adaption processes (both studies).
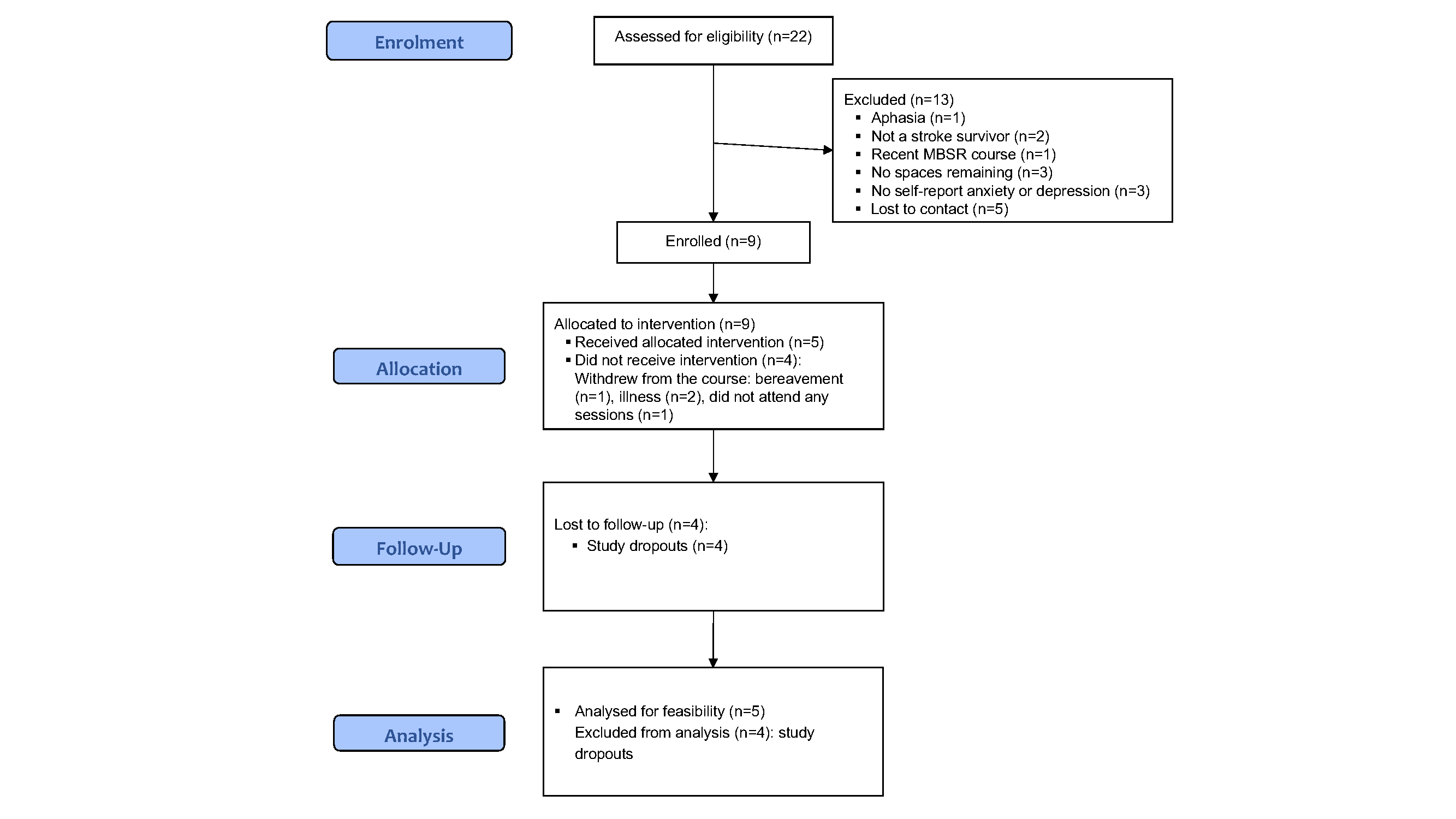
Study 2: HEADS: UP online delivery
In Study 2 we tested feasibility and acceptability of the HEADS: UP Online intervention and research processes in a non-randomised study, aiming to answer the question: what elements of design, delivery, and study processes require to be optimised ahead of a HEADS: UP Online RCT?
The structure of the intervention was unchanged from Study 1. It was delivered online, via the communication platform, Zoom©. Changes to course materials and their delivery included providing the manual in its entirety in week 1 (paper/electronic, according to preference), and uploading audio resources to HEADS: UP’s online Padlet© noticeboard after each weekly session. HEADS: UP Online was delivered by only one experienced MBSR trainer. The trainer had delivered HEADS UP in-person in study 1, having previously undertaken TtT training. As before, the trainer recorded divergence from session plans and provided feedback to enhance future delivery.
We recruited using a continually expanding community-based strategy e.g. professional and other networks, dedicated stroke/rehabilitation FaceBook groups, and Twitter. A novel feature of this was the use of short ‘recruitment’ videos made by stroke survivors and family members who had participated in Study 1 [40]. We aimed to recruit 10 stroke survivors. Inclusion/exclusion criteria were broadly similar; however, to reduce participant burden we replaced HADS with the Patient Health Questionnaire-4 (PHQ-4) [[41] and MoCA [27] and BADS with the Modified Telephone Interview for Cognitive Status (TICS-M) [42].
{kind=link}
{kind=link}