Study population
We included consecutive adult patients hospitalized in the University Hospital, Wroclaw (Poland), between March 2020 and May 2021, with COVID-19 confirmed by polymerase chain reaction testing of a nasopharyngeal sample or a positive blood antigen test. The patients were divided into two groups according to antiplatelet treatment status.
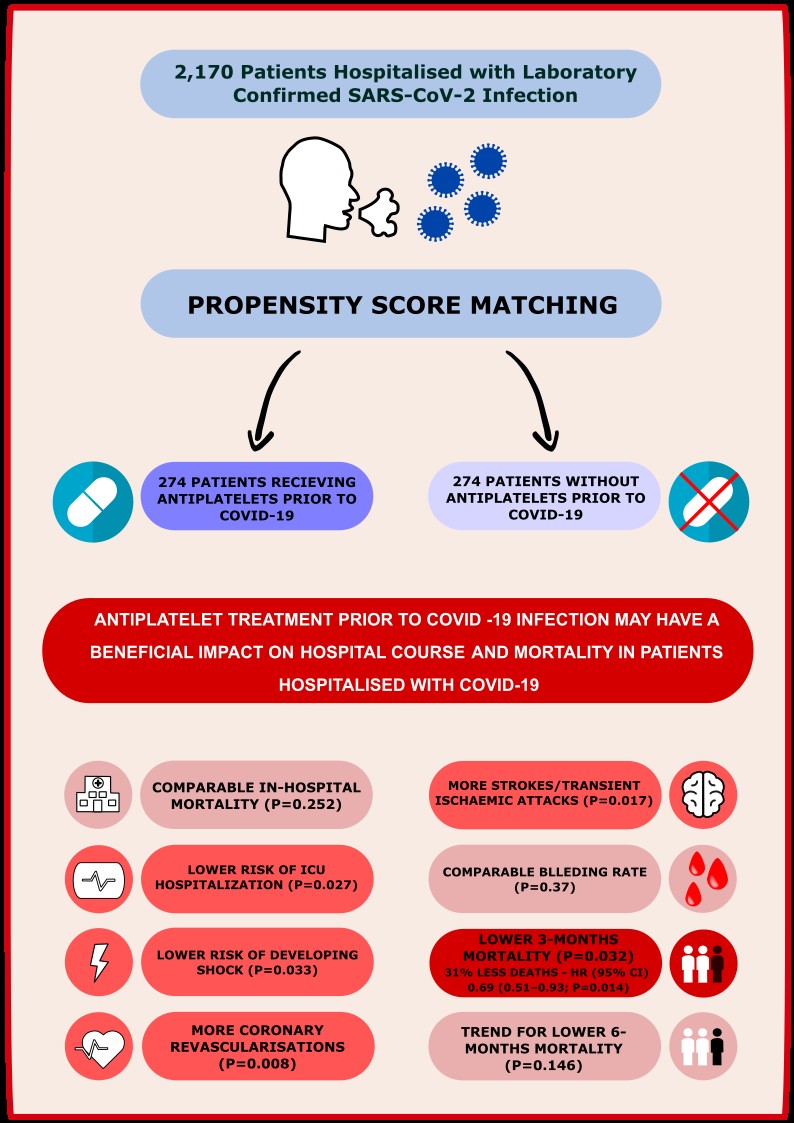
a) Patients receiving any antiplatelet treatment (aspirin and/or clopidogrel/ticagrelor/prasugrel) prior to COVID-19 infection (AP group)
b) Patients without antiplatelet treatment (non-AP group).
Patients were matched 1:1 across each cohort on a propensity score generated by the logistic regression model, adjusting for the following covariates: age, sex, arterial hypertension, heart failure, previous ischemic stroke, renal insufficiency, obesity (body mass index ≥ 30 kg/m2), diabetes mellitus.
Data Sources
Analyzed variables (demographics, laboratory measurements, comorbidities) were retrospectively collected from the electronic hospital system. The study protocol for the COLOS (COronavirus in the LOwer Silesia registry) study has been approved by the Institutional Review Board and Ethics Committee at the Wroclaw Medical University, Wroclaw, Poland (No.: KB-444/2021). The Bioethics Committee approved the publication of fully anonymized data. Written informed consent to participate in the study was waived to limit unnecessary contact and transmission of the virus. All methods were performed in accordance with the relevant guidelines and regulations. Patients who survived were followed up by telephone contact after three and six months. The patients who were contacted for their data regarding outcome gave the oral informed consent at discharge. Information regarding medium-term outcomes was obtained directly from patients, their relatives, the hospital system, and from Government General Registry Office.
Endpoints and Outcomes
The medium-term clinical outcomes were defined as 3-month, 6-month all-cause mortality. Data regarding in-hospital outcomes were also collected: in-hospital mortality, duration of hospitalization, pneumonia, admission to intensive care unit (ICU), shock, myocardial infarction (MI), thromboembolic disease, stroke/ transient ischemic attacks, acute heart failure, and all-type symptomatic bleeding. We have also analyzed the applied treatment and procedures during hospitalization, including ventilation type: passive oxygen therapy, non-invasive ventilation (high-flow nasal cannula, continuous positive airway pressure, biphasic positive airway pressure), mechanical ventilation, and the need for intubation and invasive mechanical ventilation, therapy with catecholamines, extracorporeal membrane oxygenation (ECMO), coronary angiography and revascularization and medical treatment used.
Statistics
Categorical variables were presented as numbers and percentages, the numerical variables as the mean, and standard deviation for normally distributed variables, whereas median with interquartile range (IQ) for non-normally distributed variables. The Shapiro–Wilk test was used to verify the distribution of continuous variables, and the Mann–Whitney U test was applied for group comparison. The chi-square test or Fisher’s exact test was used to compare qualitative variables.
To compare the risk of death among patients with or without prior antiplatelet therapy, we conducted a propensity score matching (PSM) using the match function of the MatchIt R package. The function parameters were set to the logistic regression model, with adjustments for the covariates. Patients were matched 1:1 across each cohort on a propensity score using the nearest neighbor technique. Balanced pairs of patients in relation to variables that could impact the outcome were selected from the entire population of 2168 patients.
The survival chances for in-hospital, 90, and 180-day follow-up, including differences between AP and non-AP groups, were checked using the chi-square test. Kaplan–Meier curves with time to death were constructed to estimate the effect of antiplatelet treatment on all-cause mortality. Differences in survival rates were tested with the log-rank test. For the doubly robust estimation, the associations between survival and potential clinical confounder, including other medical treatments, were tested using the univariable and multivariable Cox proportional hazard regression model. The univariable model was performed on the variables (demographics, co-morbidities, clinical signs and symptoms at admission and treatment applied before and during hospitalisation) that showed significant association with mortality in COVID-19 in previous studies (age, gender, BMI), which differed between the AP and non-AP groups and which were not interdependent. The multivariable model included variables that were statistically significant and associated with univariable models.
All analyses were performed using Statistica v.13.3 (TIBCO Software Inc., Palo Alto, CA, USA) except PSM, which was performed with the MatchIt R package. The P values < 0.05 were considered statistically significant.
{kind=link}