Response rate
A total of 180 clinicians participated in the survey with 74 from primary care (general practitioners) (response rate 21.1%) and 106 from hospital care (physicians and surgeons) settings (response rate 29.4%). Our response rate is consistent with many other international and Australian studies conducted with a clinical workforce. The literature reports a 30-70% response rate; however, lower than 20% has also been reported [22-25]. A national longitudinal survey of medical professionals in Australia reported an overall response rate of 19.36%, with 17.6% of GPs replying and 22.3% of specialists [26]. Missing values for questions ranged from 8.9% to 16.4%.
Characteristics of study participants
Participant demographic characteristics are described in Table 1. The majority (66%) were males and aged between 35 – 54 years (47%). Most respondents (42%) had 11-20 years of experience working in the healthcare sector. More respondents (56%) resided in the eastern states of Australia.
Table 1 Characteristics of study participants
|
Characteristics
|
N=180 (%)
|
|
Gender
|
|
|
Male
|
118 (66)
|
|
Female
|
62 (34)
|
|
Age-group
|
|
18-34 years
|
61 (34)
|
|
35-54 years
|
84 (47)
|
|
55 years and over
|
35 (19)
|
|
Years of experience
|
|
1-10 years
|
57 (32)
|
|
11-20 years
|
75 (42)
|
|
More than 20 years
|
48 (27)
|
|
Care setting and type of practice
|
|
Hospital(s)
|
Public
|
44 (24)
|
|
Private
|
14 (8)
|
|
Mixed
|
35 (19)
|
|
|
Total
|
93 (51)
|
|
Primary care
|
Private
|
15 (8)
|
|
|
Community clinic
|
11 (6)
|
|
|
Hospital-based clinic
|
12 (7)
|
|
|
Mixed
|
25 (14)
|
|
|
Total
|
63 (35)
|
|
State and territory, Australia (n=139)
|
|
Eastern (ACT/NSW/Qld/Tas/Vic)
|
101 (73)
|
|
Central (SA/NT)
|
21 (15)
|
|
Western (WA)
|
17 (12)
|
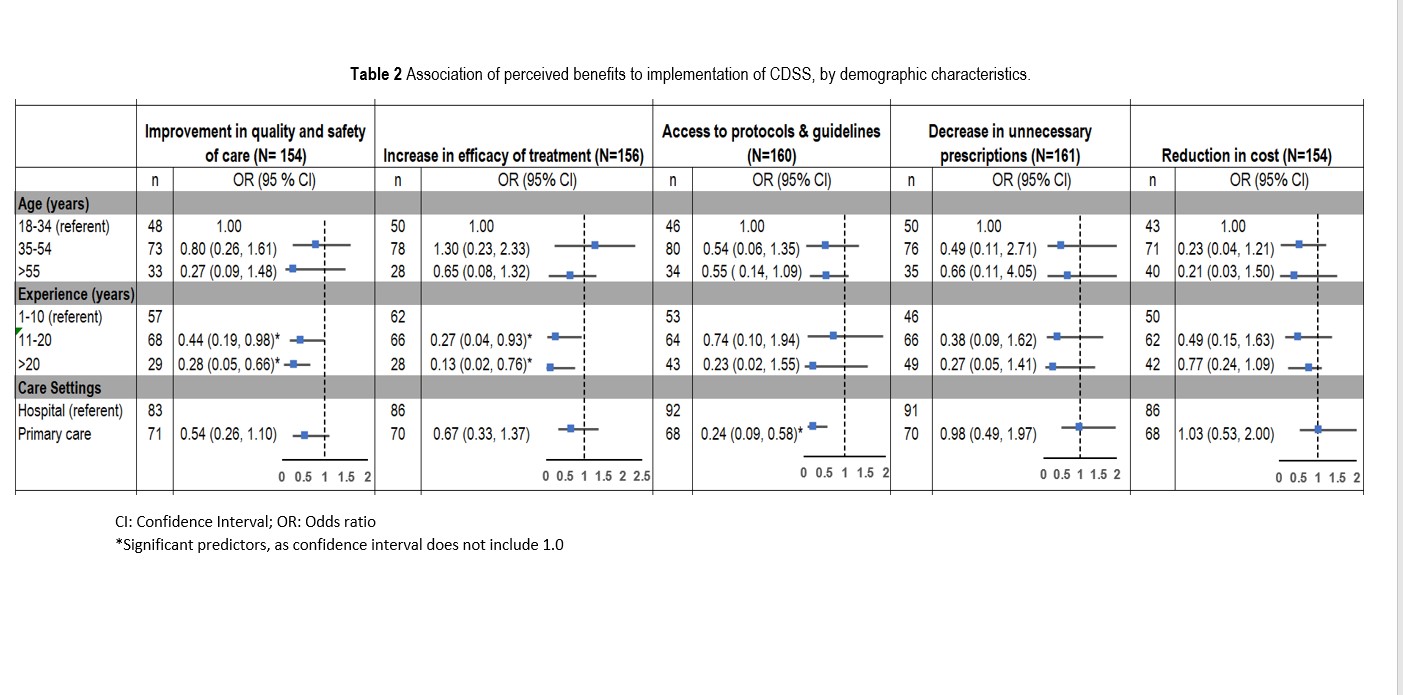
Perceived benefit of CDSS
Overall, respondents had access to a variety of electronic systems/modules, with 76% having patient information management (PIM) systems in their practices, 69% medication management (EMM) systems, and just over half (52%) had any form of clinical decision support system (CDSS) available for their use. Of all the respondents who had access to CDSS in their practices, there was a higher proportion accessing them in primary care (62%) than in hospital settings (38%).
In terms of perceived benefits, approximately half agreed (48%) that CDSS can help in reducing the overall cost of antibiotic therapy leading to more cost-effective treatment (Fig. 2). This contrasted with 79% of respondents who agreed that implementation of CDSS can increase the accessibility to information for optimal decision-making (Fig. 2). However, as shown in Table 2, this latter association was strongly associated with healthcare setting. Clinicians in primary care were 76% less likely than those in hospital settings to believe that accessibility to protocols and guidelines can be improved through CDSS use (OR 0.24, 95%CI 0.09, 0.58). Clinicians in primary care were half (OR 0.54, 95%CI 0.26, 1.1) as likely as hospital clinicians to believe that CDSS has the potential to improve the overall safety and quality of care, although this varied with respondents’ work experience. In comparison to the referent category (1-10 years), respondents with clinical experience of 11- 20 years, and >20 years were 56% and 72% respectively less likely to believe that CDSS can have any positive impact on quality and safety of care (experience 11 – 20 years: OR 0.44, 95% CI 0.19, 0.98; experience >20 years: OR 0.28, 95% CI 0.05, 0.66) (Table 2).
There was variability in responses overall, with several associations having wide confidence intervals.
Fig. 2 Overall perceived benefits of CDSS
CI: Confidence Interval; OR: Odds ratio
*Significant predictors, as confidence interval does not include 1.0
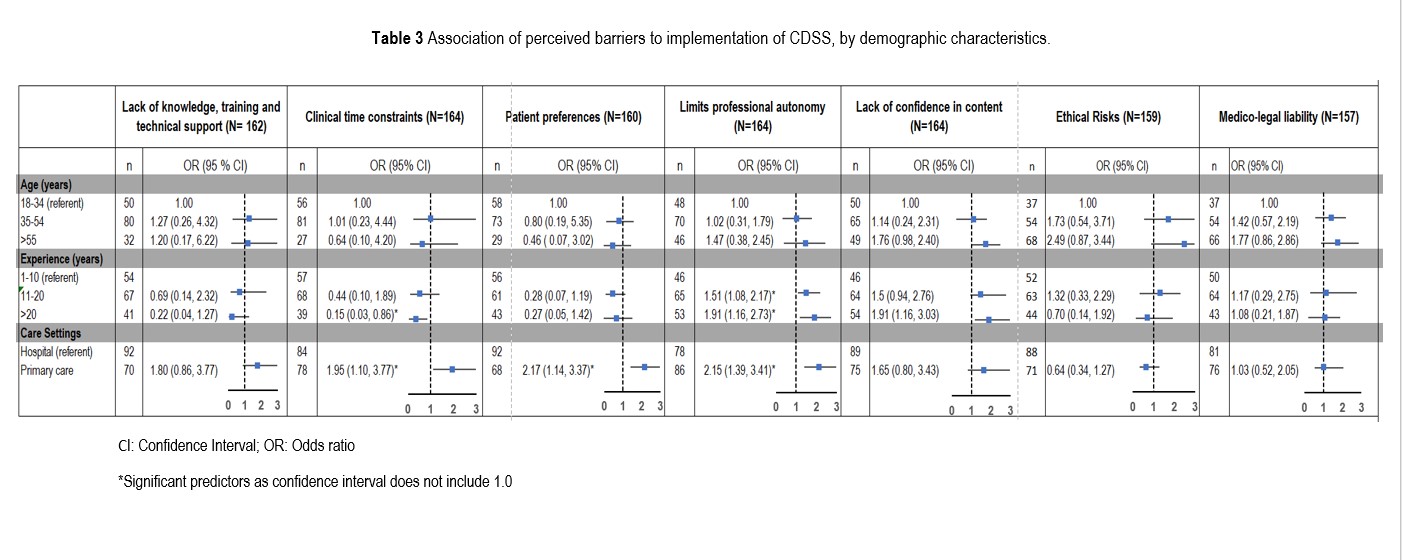
Perceived Barriers
Respondents’ perceptions regarding different factors that can impact CDSS adoption are shown in Fig. 3. Of all respondents, 69% indicated lack of technical knowledge and training are an important barrier for CDSS adoption. On the other hand, 63% of respondents believed that end users’ lack of trust and confidence in the content of the system limits the usability of CDSS. Other frequently identified barriers that may make it difficult for end-users to interact with CDSS effectively concern the dynamics of the clinical environment (Fig. 3).
As shown in Table 3, type of healthcare setting was significantly associated with clinician’s perceptions regarding certain barriers such as time constraints, limits on professional autonomy, and patient preferences toward CDSS. Clinicians in primary care settings were twice as likely as hospital clinicians to believe that time limitations (OR 1.95, 95%CI 1.10, 3.77), threat to professional autonomy (OR 2.15, 95%CI 1.39, 3.41) and patients’ preferences (OR 2.17, 95% CI 1.14, 3.37) will restrict the use of CDSS. Moreover, the likelihood of perceiving limited professional autonomy as a barrier was also found to increase with clinical experience (11-20 years: OR 1.51, 95% CI 1.08, 2.17; > 20 years: OR 1.91, 95% CI 1.16, 2.73) (Table 3). We found that 71% of respondents in primary care had clinical experience of >11 years compared to respondents in hospital settings (54%). Therefore, the association of healthcare settings with threat to professional autonomy as a barrier may be related to a higher proportion of experienced respondents in the primary care group. Overall, experienced clinicians were also more likely to believe that lack of confidence in the content of the CDSS would inhibit its use (>20 years OR 1.91, 95%CI 1.16, 3.03).
CI: Confidence Interval; OR: Odds ratio
*Significant predictors as confidence interval does not include 1.0
Fig. 3 Reported barriers to CDSS adoption.
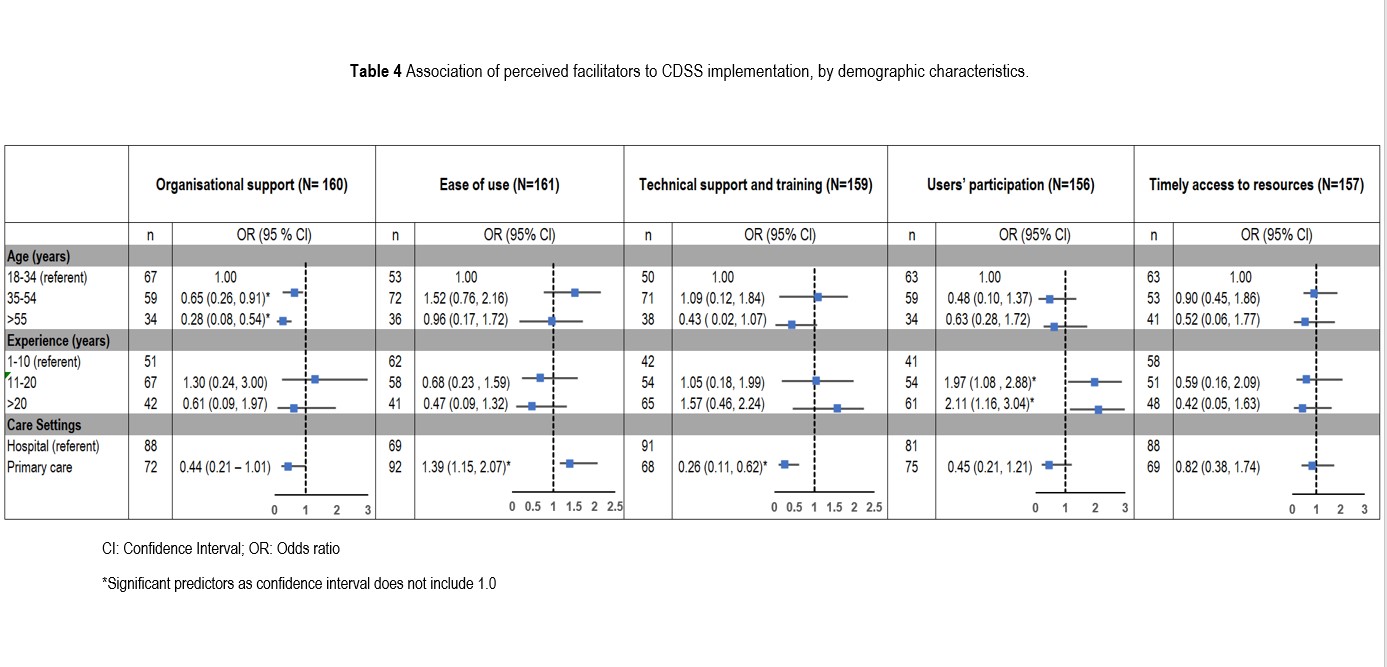
Perceived Facilitators
Figure 4 highlights strong agreement (75%) among respondents that when systems are easy to use this facilitates CDSS adoption whereas 64% believed that organisational support is required for successful implementation. Along with organisational support, 61% also agreed that effective training and technical support ensures clinicians receive adequate technological support and skills to use CDSS effectively. Stakeholders’ consultation to ensure systems are more adaptable to specific users-requirements was also cited as an important facilitator by 60% of respondents.
Healthcare setting was identified to be significantly associated with perception of certain factors as enablers to CDSS adoption. Compared to hospital settings, respondents working in primary care settings were 39% more likely to believe that ease of use will facilitate CDSS adoption (OR 1.39, 95% CI 1.15, 2.07). However, the view that technical training will improve adoption and use of CDSS was less likely to be held among primary care respondents (OR 0.26, 95%CI 0.11, 0.62). Clinical experience by length of time was a significant predictor for perceiving stakeholder consultation as an important facilitator to CDSS use. Those with greater than 11 years of experience were more likely to consider stakeholder participation as a facilitator in comparison to reference category of 1-10 years of experience (experience 11-20 years: OR 1.97, 95% CI 1.08, 2.88; experience > 20 years: OR 2.11, 95%CI 1.16, 3.04). In contrast, compared to younger clinicians (18 – 34 years) those aged 35+ years were less likely to consider organisational support as an enabling factor for CDSS adoption (age 35 – 54 years: OR 0.65, 95%CI 0.26, 0.91; age 55> years: OR 0.28, 95% CI 0.08, 0.54) (Table 4).
Fig. 4 Facilitators to CDSS adoption
CI: Confidence Interval; OR: Odds ratio
*Significant predictors as confidence interval does not include 1.0
Qualitative Analysis
Analysis of free-text comments provided three major themes related to factors that influence CDSS implementation:
i. Lack of flexibility
Respondents expressed concerns regarding CDSS inflexibility to change and cited it as a barrier to CDSS adoption. They reported that system usefulness is significantly limited if it lacks the ability to reflect the complex clinical context by taking into consideration setting and patient-specific factors:
“Systems I have experienced are comically bad in design mainly because they are inflexible in its ability to change “(Hospital)
Clinicians require flexibility and adaptability in systems instead of “constant rule-making” to tailor recommendations to specific context.
“There is never a ‘one size fits all’. So there must always be room to make exceptions” (Primary care)
ii. Information overload
“My major frustration with it [CDSS] in terms of antibiotic therapy is the presence of excessive allergy alerts, which do nothing to protect patients and simply lead to alert fatigue.” (Hospital)
Information relevance and precision emerged as important factors that influence CDSS adoption. Respondents indicated that excessive information with low specificity and relevancy leads to alert fatigue and override, thereby reducing the overall use of CDSS. Furthermore, it was highlighted that time and workload pressures make it difficult for clinicians to distinguish important information from irrelevant data.
iii. Information accuracy
“I, as a user, need to know on what basis any recommendation is provided, what is the source of this knowledge and how often it is updated” (Primary care)
The accuracy of the content was also identified as an important theme for clinicians to trust using CDSS. Respondents expressed doubts concerning the currency and reliability of the content which determines their overall trust in the system.
“…without knowing how often guidelines are updated in the system, we cannot rely on system alerts” (Hospital)
The uncertainty felt by clinicians about the quality and accuracy of evidence negatively impacts their perception of CDSS.
{kind=link}
{kind=link}
{kind=link}