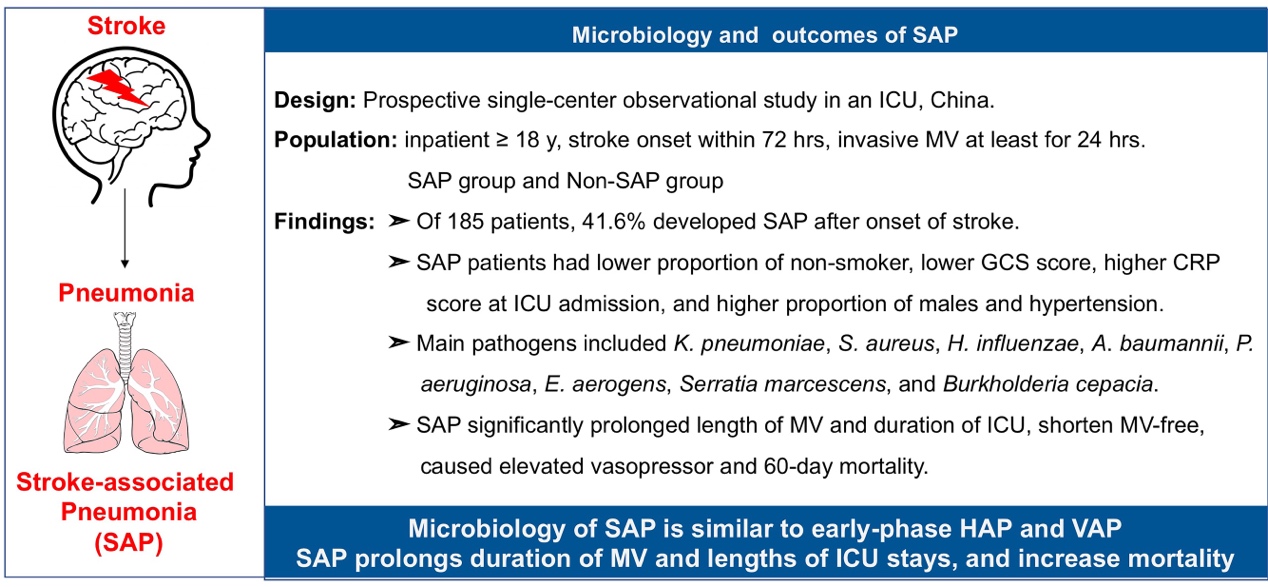
This was the first survey investigating microbiology of SAP in LRT for post-stroke patients treated with invasive MV. In our study, the main attributed pathogens were K. pneumoniae (39%), S. aureus (26%), H. influenzae (10.4%), A. baumannii (7.8%), P. aeruginosa (6.5%), E. aerogens (5.2%), Serratia marcescens (5.2%), Burkholderia cepacia (5.2%), similar to the microbiology of culture-positive pneumonia for hospitalized neurologic patients and early-onset VAP[19–21]. Besides, a systemic review involving 7968 patients with acute stroke indicted that the commonly isolated organisms of SAP included K. pneumoniae (12.8%), E. coli (9%), S. aureus (10.1%), P. aeruginosa (6%), A. baumanii (4.6%) and S. pneumoniae (3.5%)[22]. As for the type of pathogens, our conclusion was of essential agreement with the systemic review, however, the specific frequency for each pathogen calculated by different studies varied. This difference might be explained by many divergences among studies including heterogeneity of patients’ population, heterogeneity of epidemics in different region, heterogeneity of clinical environment, whether treated with invasive treatment or prophylactic antibiotic therapy (PAT) and so on. For instance, this systemic analysis pointed out that studies whose patients were at relatively higher-risk such as dysphagic or ICU admission had a high proportion of Gram-negative aerobic bacilli and S. aureus, which is consistent with findings in our study[22].
Critically ill patients deserve more attention, as they have many risk factors of SAP, including hypertension, dysphagia, MV, male, a lower consciousness level and bedridden[23]. In our study, hemorrhagic stroke was the main type of stroke. Actually, ischemic stroke is the more common type of stroke, and most researchers always recruited patients from stroke units (ischemic stroke predominated) or directly selected patients with ischemic stroke[22, 24, 25]. The difference between ischemic stroke and hemorrhagic stroke was lying on many aspects including mechanism, symptom as well as prognosis, whereas whether these divergences would further impact SAP are still unclear. For example, stroke-induced immunodepression was found correlated with mechanism and morbidity risk of SAP for patients with ischemic stroke[26, 27]. However, whether immunodepression induced by hemorrhagic stroke is identical to ischemic stroke still uncertain. In our prospective cohort study, serum CRP and PCT, increased vigorously comparing with the baseline level at ICU admission. Serum CRP and PCT were considered to be independently associated with SAP in some studies, but not others. The diagnostic value of serum CRP and PCT in discrimination of SAP was not definite yet[28]. Improvement of diagnostic sensitivity and specificity need comprehensive consideration of symptoms and biomarkers. For afebrile patients with chest findings and leucocytosis or new radiological chest infiltrates, Kalra et al highly recommended CRP ≥ 30 mg/L as a supplement to diagnosed SAP[29]. This strategy remedied missed diagnosis owing to afebrile to some extent. In our study, CRP at ICU admission elevated mildly in SAP group (10.6 vs 5.2 mg/L, p < 0.001) than non-SAP, which might be a somatic response to acute stroke or correlate with stroke-induced immunodepression. However, whether such CRP change in early phase was a valuable sign helping recognize potential patient with SAP, are still unknown. In addition, dynamic change process of biomarkers (eg. CRP and PCT) reflect the progression and prognosis of disease to some extent. PCT were considered to have higher diagnostic and prognostic accuracy of SAP than CRP in recent studies[30, 31]. Interestingly, PCT-guided antimicrobial strategies in ICU attracted a lot attention, and PCT-guided cessation of antibiotics were found to reduce both antibiotic exposure and mortality[32, 33]. PCT might be a good indicator reflecting progression of SAP and guiding clinical medication. More studies should be designed to clarify the details about role of the serum CRP and PCT in SAP. We found patients with SAP spent more time on MV and staying in ICU, were applied more vasopressors, and had higher 60-day mortality than patients with non-SAP. This conclusion is consistent with the findings in previous studies, in which SAP was associated with poor functional outcome and mortality[34, 35]. It is really important to figure out how to recognize potential patients as early as possible and how to take active strategies to avoid the occurrence of SAP.
Some patients were applied antibiotics before operation because they indeed faced high-risk of infection and had a poor physical status in our study. Although antibiotics use was discouraged to prevent SAP according to current guidance, physicians still would choose PAT in practical clinical work, considering the infectious threat patients faced and low probability of victory of anti-infection only relying on themselves. Whether PAT favors preventing infection and prognosis is a controversial topic, and several studies have been performed[18, 36–38]. Two multicenter, open-label, randomized controlled trials with masked endpoint assessment have been published. The Preventive Antibiotics in Stroke Study (PASS) conducted by Westendorp et al explored the positive effects of ceftriaxone on outcomes for patients with acute stroke, whereas Lalit et al investigated whether prophylactic antibiotics could reduce pneumonia in post-stroke patients with dysphagia (STROKE-INF)[18, 37]. The former found PAT could reduce incidence of infection, while the latter illustrated that PAT did not reduce the frequency of pneumonia. The consistent conclusion in these two high-quality studies was that PAT did not improve functional outcome at 3 months. The above findings suggested PAT was only capable of preventing urinary tract infections, not SAP[39]. In summary, in terms of bactericidal effect of antibiotics, no antibiotics have been found to have beneficial effects in preventing SAP so far. However, specific antibiotic protocols in each study succumb to local hygiene policies based on local epidemiology, and influenced by local empiric administration habits. Several factors such as type of antibiotics, time point of administration, dose, mode of administration, type of population will impact the final effects of antibiotics. We haven’t found the positive effects of PAT in SAP so far, probably because we didn’t choose the optimal antibiotics strategies in previous studies. Another point attracted our attention is the neuroprotective effects of some antibiotics. Previously, ceftriaxone was found to significantly reduce acute stroke mortality in animal models, and these positive results might be due to its neuroprotective effects including increasing glutamate uptake and inducing neurotrophins[40]. Recently, Dai et al found that minocycline could attenuate brain injury and iron overload after intracerebral hemorrhage in aged female rats[41]. Besides, Yang et al also demonstrated that minocycline could attenuate acute stroke injury in rat brain by promoting blood–brain barrier remodeling and facilitating neuroprotective phenotype alternative activation of microglia / macrophages. Treatment with minocycline significantly reduced levels of pro-inflammatory factors tumor necrosis factors-α (TNF-α) and interleukin-1β (IL-1β) and increased levels of anti-inflammatory factors transforming growth factor-β (TGF-β) and interleukin-10 (IL-10)[42]. As we all known, neurovascular injury is the primary etiology of SAP, antibiotics would have application value in early phase of stoke if they have neuroprotective effects. Thus, this direction needs more attention and more investigations should be conducted to clarify more details. In summary, it is insufficient to totally negate the effects of PAT in SAP just depending on evidence from current studies.
There are some limitations in our study. Firstly, our study is single-center observational cohort study and the sample size was relatively small. Since microbiology of SAP associate with local epidemiology, our findings need to be further validated in a larger cohort based on multi-center cooperation. Secondly, our study only focused on patients’ short-term outcomes such as duration of ICU stays and 60-day mortality. Long-term follow-up should continue to figure out the effects of SAP in long-term outcome. Thirdly, as microbiologically confirmed bacterial pneumonia was the focus in our study, determination of infection strictly followed results of sputum bacterial culture, whereas virus detection was not performed in our study. It would be better when broader pathogen (eg. bacterium and viruses) distribution and frequency were figured out. Finally, some patients were applied pre-operative prophylactic antibiotics since they had high-risk of infection and serious status, which might impact the results of bacterial culture. The main antibiotics in our study was cefuroxime, which is a broad-spectrum antibiotic. Thus, the actual morbidity of SAP might be higher than results obtained in our study.
{kind=link}