Histological changes caused by HCC are varied in different patients that cause enormous problems in diagnosis. Therefore, accurate detection methods are necessary to assuredly diagnosis of HCC in an early stage.
HepPar-1 is one of the key factors in the urea metabolism cycle and can be highly sensitive and specific in detect of hepatocytes (16). Arg-1 is mainly produced in the liver tissue, the main objective of this study was to evaluate the expression pattern of Arg-1 and HepPar-1 in patients with liver cancer (17).
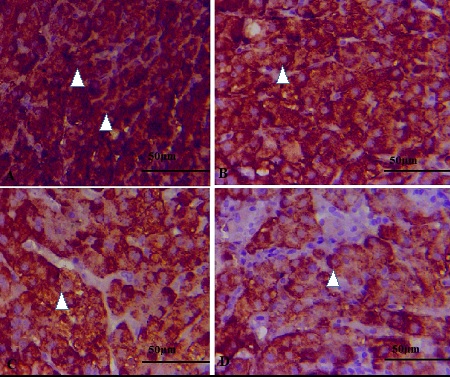
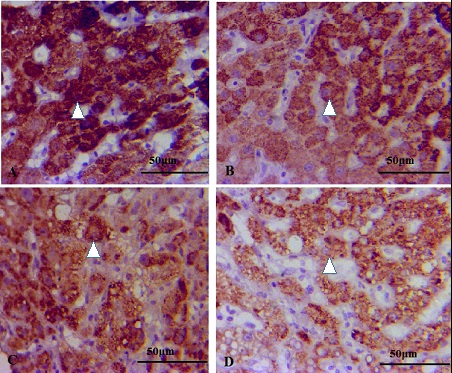
The staining pattern of hepatocytes by Arg-1 was mainly diffuse cytoplasmic and patchy nuclear reactivity, both in normal and HCC liver samples. Given that the role and function of Arg-1 in the nucleus are unknown and its expression is poor, in many studies scientists neglect it and only consider the expression of Arg-1 in the cytoplasm (18).
In the current study, HBV infected patients with HCC had significant lower levels of HepPar-1 and Arg-1 than patients with only HBV infection. These proteins can partially determine the likelihood of cancer in people with hepatitis B infection. The expression of HepPar-1 and Arg-1 is associated to the risk of HBV-related HCC, as both of them have been reduced in patients with HBV + HCC. Also, Arg-1 was more specific and sensitive than HepPar-1 and could be a more suitable biomarker for increase the specificity and sensitivity to an acceptable level.
As revealed by the findings of this study, in all groups, Arg-1 has been shown to be more sensitive to detection of cancer than HepPar-1. The results in the field of HepPar-1 function in cancer diagnosis are almost similar to those of other studies, Fan et al. (19), Fu et al. (20), Wang et al (10) and Benjamin et al. (18). On the other hand, all cancer patients showed a diagnostic response to both proteins and apparently, Arg-1 can easily and reliably replace HepPar-1 in cancer diagnostic processes. Studies by Yan et al. (18) and Dana et al. (21) also confirm this hypothesis.
The Arg-1 specificity in the diagnosis of cancer was somewhat higher than that of HepPar-1. So, diagnosis of HCC by HepPar-1, must be handled with care. Given that, distinguishing of HBV-related HCC in early stages is crucial, therefore in order to confirm the diagnostic specificity of Arg-1 rigorously, the expression level of both proteins was evaluated especially in the groups that were potential prone to HCC, including HBV infected patients. Of note, healthy controls often express HepPar-1 in a way that Fasano et al. have found that it was produced in subjects without HBV or HCC (22).
Our findings in current study indicate the important diagnostic specificity of Arg-1 in cancer patients on fine-needle aspiration specimens. Also, Arg-1 evaluation showed that this protein could be highly sensitive in identifying hepatocytes (18). Furthermore, proper combination of HepPar-1 and Arg-1 improved the accuracy of cancer detection in people with hepatitis B which can helpful in disease control. HBV patients with cancer were diagnosed with a 100% specificity, when using a combined model of Arg-1 + HepPar-1. One of the complex issues in the detection of liver malignancies is diagnosing hepatic failures which are susceptible to advanced stages of liver disease. In this study, the Arg-1 antigen partially resolved this problem using an immunohistochemical panel because it was able to be expressed as a specific marker of hepatocyte cells in all groups with a clear pattern.
Another point that was highlighted by the findings of this study was that the combined model included Arg-1 + HepPar-1, improved the process of cancer diagnosis of HBV-related HCC, especially in fine-needle aspiration samples with too small cell count to evaluate the status of the sample and disease.
{kind=link}
{kind=link}