Adequately deep plane of anesthesia was found at the time of eccentric fixation of eyes in down gaze on all occasions in our study. This was demonstrated by the higher value of MAC in all cases. Eye score (-4 to +4) showed a significant negative correlation with DOA, thereby confirming elevated eye position with lighter anesthesia and downward eye position with a deeper level of anesthesia.4,7 In his study under different depths of general anesthesia, Power et al13 observed final eye position in downward direction in few patients but their number, DOA, and down-scoring of eye position were never described. In his study of 32 patients, Kook et al2 scored the vertical position of each eye on an ordinal scale from -2 to +6, according to its height in relation to the medial canthus, and studied the relationship between fixed eccentric eye elevation and DOA during surgery in 32 children. He encountered elevation of the eyes in 83%, and downward position of eyes was in 2% (1 child) with BIS values less than 35.2 BIS was performed only in 5/14 surgeries in our series. Though values of BIS in infants and young children do not indicate a similar concentration of sevoflurane like adults,14 lower values of BIS generally indicate deeper level of anesthesia. Lower values of BIS corroborated deep anesthetic level in 3 events, but BIS values did not corroborate the DOA during the other 2 events. (Table1) which could be understood with the fact that BIS values are not validated in small children and hence may not be always reliable.
This tonic downward movement was seen in pediatric cases under sevoflurane GA in absence of muscle relaxant (or when effect of NDMR waned off in one case) when attempts were made to rapidly deepen/optimize the plane of anesthesia (on surgeon’s request to centralize eye position from eccentric positioning in up-gaze) or before the start of surgery when eyes were opened after cleaning and draping procedure following handing over the anesthetized child to ophthalmic surgeon by the anesthetist when or after the start of surgery when traction was relaxed in-between. Power et al13 while studying the DOA in young adults via sevoflurane induction compared eye signs with EEG polysomnography and showed that, the deepest level of sleep was reached on an average 3 minutes before the onset of eccentric ocular positioning thereby suggesting that eccentric eye movements may occur even when a patient appears satisfactorily anaesthetized. This also points towards understandable lag between anesthetic depth reached at the level of lungs and its effect seen at the level of CNS (eccentric eye positioning). This could be the possibility, as most of our patients experienced downward movement at or before the start of surgery. During induction sevoflurane flow to lungs is generally kept high (MAC is kept high during induction barring the level of apnea) and then slowly decreased to desired level once the child gets anesthetized which is continued even after handling the child to ophthalmic surgeon. Rapid induction might overlap this lag with short duration surgeries when most of the children witnessed downward or upward movement before/at the start of surgery, depending on DOA and child’s threshold value. Also, rapid increase in flow of sevoflurane to centralize upward eye-positions (deepen DOA) also explained rapid downward movement following upward movement (patient 1). Few children witnessed downward rolling at the end of surgery at the same MAC, surgery was performed, and the probable reason could be that DOA (although MAC was kept constant) varies with the level of stimulus (like traction on eye) the patient is experiencing. This may be illustrated by the fact that one of our patients experienced downward movement at the end of surgery (during conjunctival suturing) on the same MAC (1.3) eyes were central and was being operated upon.
In 1848 Snow15 defined the cessation of voluntary eye movement and a slight inclination of eyes in up-gaze as the point of sufficient anesthetic depth. Rossiter et al3 reported its substantial increased incidence without the use of muscle relaxants. Higher incidence of up-gaze eccentric movement (34.4%) in Kook’s study2 was due to an extended duration of the measurement period, including the time of emergence from anesthesia as upward eye positioning is more commonly seen at the end of surgery when anesthesia is lightened. In our case series also upward drifting of the eyeball was seen under lighter planes of anesthesia during eye manipulation during surgery as demonstrated by lower MAC values (median 1.0) in 5 patients in which upward drift was seen during surgery. The high BIS value (55) recorded in case1 corroborated the findings of the prior studies.4,7
Inhalational agents are known to cause a dose-dependent suppression of reflexes and movements.5 Complete lack of electrical discharge in the extraocular muscles occurs only during deep sleep or deep anesthesia.5 But the increased DOA is not always effective in reducing eye movements.13,16 Moreover, different anaesthetic agents may have different effects on eye movements.17 Presence of electrical activity in one of the extraocular muscles occurs over its opposing muscle in the lighter plane of anesthesia, and probable causation has been discussed in the literature by many researchers. Rossiter et al reasoned intense and sustained contraction of superior rectus (SR) behind the eccentric upward eye position.3 Harrad and Stoddart18 suggested that Bell’s phenomenon, a natural protective reflex, in which the globe rolls up in response to any noxious stimuli in the form of pressure on the globe or any manipulation of the eyeball may explain this upward eccentric eye position.19,20 This occurs both in the awake state and with lighter planes of anaesthesia (though the patient is not awake) which may explain the entity. The exact neural mechanism is unknown but involves brainstem pathways between the seventh cranial nerve nucleus in the pons and the third cranial nerve nuclear complex in the rostral midbrain. Hiraoka et al21 have suggested that the mesencephalic reticular nucleus may play an important role in integrating these two patterns of movement (bilateral lid closure and upward movement of both eyes). Bell's reflex is also extinguished with deep planes of anaesthesia, such that the eye remains in the neutral gaze.18,22 And this upward drift in cases 2, 3, and 4 prompted the anesthetist to increase the DOA to make the eyes return from the upward position following which down-rolling was encountered.
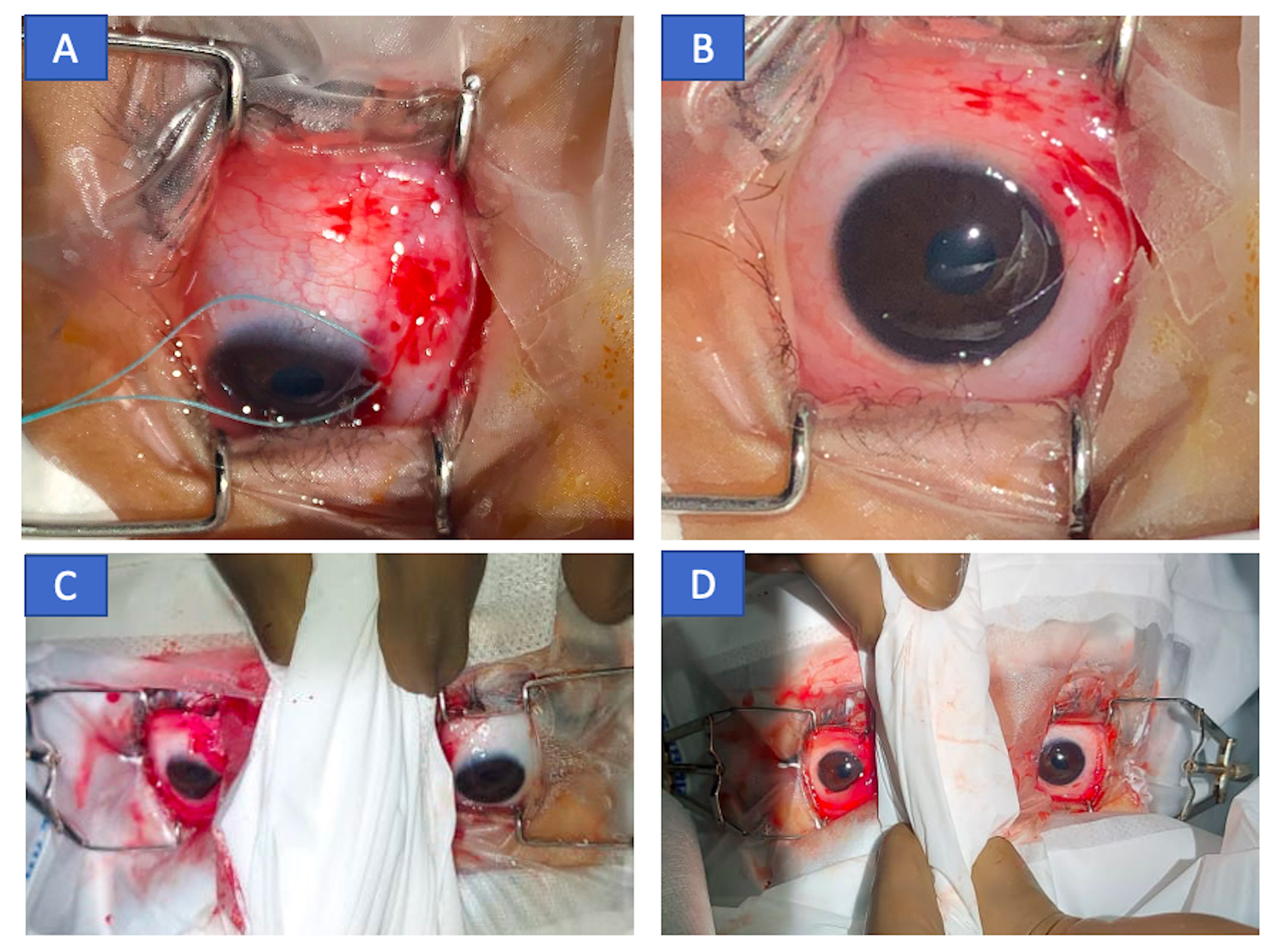
In our study, down-rolling made surgeons abandon the procedure till the time it lasted. Similarly, it appeared to have resulted from a tonic contraction of the inferior rectus of both eyes, as it was difficult to manually rotate the eyes and carry the procedure. All cases had symmetric down-rolling (Figure4) except case 6 in which asymmetry was evident (Figure3). Though we could not understand the exact reason of asymmetry, but we suspected asymmetric dissociated vertical deviation in the child to alter the eye position.
Probable pathophysiology behind downward drift
The pathophysiology of down-rolling under GA is unknown. We tried to hypothesize based on the shared neurochemical and behavioral features of sleep and general anaesthesia.23,24,25 Various anesthetics have been demonstrated to alter brain systems involved in sleep-wake control.24,25,26,27 Many medicines produce general anesthesia that is very comparable to NREM sleep28, including a breakdown in efficient cortical communication29,30 and inactivation of the thalamus and midbrain reticular formation along with loss of awareness.31,32 Anaesthetized patients' brains may be trapped into an NREM-like state, preventing access to REM sleep and waking.31,33 In a wakeful state, the mesencephalic reticular development is critical in creating a vertical saccade.34 REM sleep activates cholinergic neurons in the reticular formation.35 The similar velocity-amplitude correlations of rapid eye movements during REM sleep and spontaneous saccades in the dark when awake, suggest a shared neural circuit.36 Since eye movements changed with MAC, we hypothesize that a sudden increase in anesthetic concentration (which might have been potentiated with use of sevoflurane during induction for deepening or maintenance of DOA during surgery) caused temporary irritative effects in the central nervous system, causing temporary switching37 of non-REM to REM sleep-like state or isolated REM sleep-like traits being expressed during non-REM sleep-like state38 with activation of the mesencephalic reticular formation and neurons.
The irritative effect of increased anesthetic concentration can be many-fold, although prospective studies are required to evaluate these theories.
1. An increase in sevoflurane concentration (higher MAC) and differential sensitivity of cortical and subcortical areas to sevoflurane concentrations.39 In adults, Mourisse and colleagues40 found that the blink reflex (brainstem function) was more susceptible to sevoflurane than BIS (forebrain function). The interstitial nucleus of Cajal, the mesencephalic reticular formation, and the posterior commissure are all located at the meso-diencephalic junction.41 Forced downward gaze is prominent in this area's lesions, indicating a vertical gaze plane imbalance.42 In our cases, down gaze neurons in the midbrain were possibly selectively irritated by sevoflurane.43,44 Prepubertal children's lesser sensitivity to sevoflurane for specific subcortical areas (i.e. mesencephalic control) than older subjects may explain its prevalence only in select children.39 Different flow rate of anesthetic agent used, different time taken and different DOA achieved during intubation and as well as different DOA (MAC value) on which the patient is stabilized before handing them over to the ophthalmic surgeon for the procedure, could be factors influencing the non-occurrence of eye movements during repeat exposures in the same patients.
2. Another potential reason could be related to shortened autoregulation and vasodilatory impact of sevoflurane generating transient reduced cerebral blood flow (CBF) and irritative effect which reverses when concentration is decreased.45,46 The lower limits of sevoflurane autoregulation are close to young children's basal mean arterial pressure.47 The fact that our patients' exhibited eye movements beyond 1.5 MAC supports this hypothesis, as CBF remains unchanged by sevoflurane up to 1.5 MAC value.45,48 It is possible that the CBF sensitivity window is quite narrow and specific to each individual. it is likely that the narrow autoregulation limit was violated when the depth went above the child's acceptable limit. The posterior circulation zone supplying the mesencephalic-diencephalic junction, comprises structures critical for vertical sight and vergence,49 may be transiently impaired, manifesting eye movements. The concentrations at which these downward movements were seen in our cases necessarily do not lead to cerebral ischaemia in healthy children as thousands of sevoflurane inductions are performed every day in children, and neurologic complications are quite rare. The movement occurred only when the MAC level was below or beyond the narrow limit in sensitive children.
Burst neurons and tonic neurons are the two types of saccade-generating neurons.22 Burst neurons produce high-frequency bursts of action potentials right before the eye movement, whereas tonic neurons fire at regular intervals to keep the eye in the new eccentric position. Also, pause neurons are thought to have a tonic inhibitory influence on saccadic eye movements. Because the mesencephalic reticular structure is activated, the eye moves quickly to down gaze. The ensuing tonic neuron firing may have kept the eye in the downward eccentric posture until the anesthetic wore off. The downward movement was slower than a normal saccade, since most anesthetic drugs reduce peak saccadic velocity dose-dependently.17,50 Anesthesia reduces peak saccadic velocity due to the absence of a visual target in the superior colliculus, which increases cells activity in the superior colliculus and corresponding motor pathways.
3. A third possibility is that sevoflurane is known to excite the neurons in Locus Coeruleus (LC).51 The LC is a pontine nucleus, with the largest group of noradrenergic neurons in the brain, that is responsible for the tonic maintenance of the wakeful state.52,53 This nucleus has very widespread projections to cortical, subcortical regions and to the spinal cord.54 In addition, it also projects to the oculomotor nucleus which has been shown to have a high density of α1-adrenoceptors.55,56 It is plausible that sevoflurane, at higher concentrations, induces the activation of the LC leading to the tonic contraction of the muscles innervated by the oculomotor nerve. As the LC is also involved in maintaining the wakeful state, once the DOA is on the lighter side it is possible that the same scenario of LC activation repeats itself. LC activity, through effects on α2-adrenoceptors in the Edinger-Westphal Nucleus,57,58 can inhibit pupillary constriction by attenuating the light reflex. This might be the reason why we noticed ocular movement without any pupillary change. The interindividual differences in the specificity of these projections, in addition to the fact that MAC per se has been defined for producing immobility to surgical stimulus in 50% of the population,59 may explain why these ocular movements are not noticed in every case.
The limitations of our study are a small sample size and no BIS or EEG monitoring in all participants. The limited sample size limits generalization of reported median MAC values and the usefulness of the association between DOA (MAC value) and eye-positioning score. In addition, because all observations were made after the induction procedure was completed, and the anesthetic depth was stabilized to the desired level, the incidence of downward eye positions may have been underestimated.
This article intends to educate ophthalmologists and anesthetists about this unexpected eye movement during general anesthesia. This entity is important in short ocular procedures or surgeries under GA, especially without NDMR. Our case study demonstrates the importance of keeping a stable DOA. In the event eye movement occurs, the anesthesia team should be contacted immediately, and the surgery should be restarted after the eye movements have stopped, and the eyes have returned to their normal position. Relaxants may be used for novices in ocular procedures involving critical steps like cataracts and squint. Also, more research is needed on the link between eccentric downward movement, eccentric upward movement, and level of anesthesia (using BIS and MAC values) and electrical activity of brain (Electro-encephalogram). Aside from electro-oculogram, we need to explore the tonic force in the inferior rectus to understand the pathophysiology of these eye movements, giving clues into ongoing subcortical processes. It will be fascinating to see if an anesthetic drug plays a role in these motions. Further research is required on the entity's link to anesthetic depth and age.
{kind=link}