HER2-positive breast cancer patients have poor prognosis due to the aggressive nature of HER2-positive disease [6]. Many studies have reported that HER2-targeted treatments, including anti-HER2 antibodies (such as trastuzumab and pertuzumab) and small-molecule tyrosine kinase inhibitors (such as lapatinib and neratinib), have excellent overall survival benefits in this patient cohort [1]. Therefore, determining the HER2 expression level in tumors is vital when selecting targeted therapy. Currently, this means analysis of HER2 expression by IHC and/or HER2/neu gene amplification by FISH. However, despite standardization of testing methods and interpretation recommendations, assessment of HER2 status can still be inaccurate. Several factors contribute to this imprecise HER2 interpretation, such as HER2 heterogeneity, gain in chromosome enumeration probe 17 copy number, and HER2 status alteration after neoadjuvant chemotherapy or during metastatic progression [13]. As more therapeutics are approved for HER2-postive tumors, there is a growing need to accurately determine the HER2 status of both primary and metastatic tumors.
In this study, we utilized an accurate, whole-body and non-invasive method for HER2 status determination to help clinicians to identify breast cancer patients who will benefit from HER2-targeted therapy. This first-in-human study of 99mTc-NM-02 as a radiotracer for SPECT/CT assessment of HER2 expression was conducted in 10 female breast cancer patients. The safety of this tracer was excellent, with no reported adverse reactions and acceptable radiation dosimetry. The SPECT/CT data demonstrated favorable biodistribution and satisfactory imaging characteristics of 99mTc-NM-02. As with other radiolabeled sdAbs [23–25], the urinary system received the highest radiation dose, but it was tolerable. The radiation dosimetry of 99mTc-NM-02 was similar to that of the 99mTc-labeled anti-PD-L1 sdAb reported in our previous study [26]. Although the individual organ doses are acceptable for a diagnostic procedure and in line with other 99mTc-labeled radiotracers in clinical use [29], they could potentially be further minimized by faster excretion using methods such as co-injection of diuretic agents.
Some studies have attempted to decrease nonspecific radiotracer accumulation in the liver and spleen by increasing the dose of non-radiolabeled sdAb, but the effect was very limited [24]. In our previous study, we encountered similar results [26]. In that study, we observed no significant differences in image quality, biodistribution, and tumor-to-background ratios in patients receiving 100 and 400 µg of sdAb. Therefore, we injected 100 µg of NM-02 sdAb in this study. As anticipated, the 99mTc-NM-02 tracer mainly accumulated in the liver and kidneys, and increased activity in the bladder indicated that 99mTc-NM-02 was eliminated through the urinary system, in line with the excretion patterns described in the literature [24].
Although trace uptake in the liver, spleen, and intestines was visible early after injection, we observed rapid clearance from these organs at 1 h after injection, with no signs of hepatobiliary excretion, such as an enhanced accumulation in the gallbladder or duodenum. This might be explained by the rapid clearance of 99mTc-NM-02 from the blood pool. The rapid blood clearance not only allowed us to perform SPECT imaging at early time points (within 2 h after injection) but also might reduce the risk of false-positive signals due to high activity in the blood pool. In addition, there was rapid tracer reduction in normal lung tissue, which further improved the contrast of primary breast cancer and metastases in images. Because of this continuous and rapid decreasing activity in the blood pool and lung background over time, images acquired at 2 h after injection had higher signal-to-noise ratios than those acquired at 1 h.
Unlike the biodistribution data in our previous work [26], mild uptake of 99mTc-NM-02 was observed in the thyroid, submandibular, and parotid glands. This pattern has also been reported in other studies of similar tracers, such as the 68Ga-labeled anti-HER2-nanobody and the 111In-labeled anti-HER2-Affibody [24, 30, 31]. The tracer uptake may reflect the low-level HER2 expression in these glandular tissues, or it may be associated with chelator-mediated trapping mechanisms. However, studies performed with 18F-anti-HER2-nanobody and 111In-labeled anti-HER2 monoclonal antibody showed insignificant uptake in these glands [32–34]. Notably, glandular uptake has also been reported in prostate-specific membrane antigen and fibroblast-activating protein inhibitor tracers [35, 36]. These results reveal the complex mechanisms of glandular uptake, and its cause remains unknown.
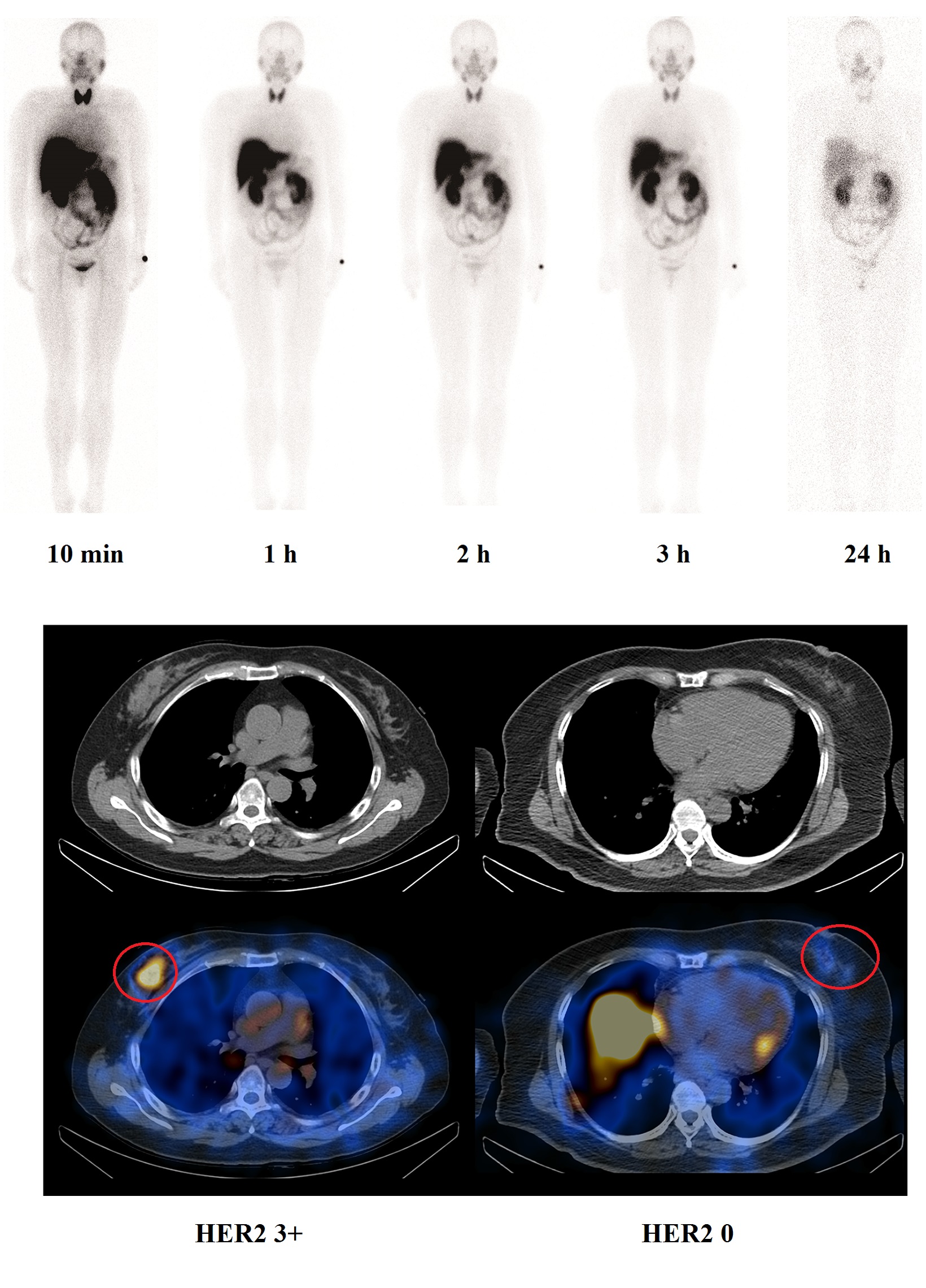
The SPECT/CT images of primary lesions and metastases were carefully evaluated in these breast cancer patients and compared with their HER2 IHC results. As expected, five patients with positive HER2 IHC results had obvious tracer uptake in their primary lesions. Remarkably, four of five HER2-negative patients in this study also showed obvious local tracer uptake in their primary tumors, likely due to the intratumoral heterogeneity of HER2 expression. This discordance in uptake might be due to the tumor specimens being obtained by core needle biopsy from a small area of the tumor, which fails to capture the heterogeneity within the tumor. Additionally, intertumoral heterogeneity was observed in some patients with metastases. Distinct uptake was seen in the metastases of seven patients, although the primary tumor of one patient (Patient BR003) was classified as HER2-negative based on pathology results. Conversely, one patient (Patient BR001) with inconspicuous tracer uptake in metastases had high HER2 expression (HER2 3+) in the primary lesion. The inconsistency of tracer uptake in metastases could be attributable to a discordance in HER2 expression between the primary tumor and the metastases, which has been previously reported [37, 38]. This intra- and intertumoral heterogeneity in HER2 expression highlights the need for the development of non-invasive imaging methods to provide more holistic information on HER2 status when making HER2-targeted therapy decisions.
Tumor uptake in the primary lesions and metastases of these breast cancer patients showed a wide range of SUVmax (0.35–11.18). Although it was not the primary purpose of this early phase I study, based on these SUVmax, we attempted to identify a cutoff for determining HER2 positivity in SPECT/CT imaging. An SUVmax of 1.5 appeared to be a reasonable point. Using this cutoff, the results of visual interpretation from nuclear medicine doctors and the tumor SUVmax at both 1 h and 2 h post-injection were consistent. Interestingly, Patient BR008 was originally identified to have a HER2-negative tumor based on imaging by visual interpretation at 1 h post-injection, but the tumor was redefined at 2 h post-injection (SUVmax of 1.36 and 1.76, respectively). This suggested not only the utility of the identified cutoff value but also the importance of delayed imaging for the patients with equivocal uptakes.
Several researchers have discussed the advantages of sdAbs as novel candidates in the development of molecular imaging tracers when compared with full therapeutic antibodies [16]. Based on these distinctive properties, many researchers have labeled various anti-HER2 sdAbs and antibodies with different radionuclides for PET and SPECT imaging, including 89Zr, 64Cu, 68Ga and 111In [23, 24, 39–41]. However, the availability and production costs of these radionuclides may hinder their rapid clinical transformation and popularization. In this situation, 99mTc-labeled sdAbs can be translated into clinical application with more ease, thanking to the ideal properties and popularity of 99mTc radionuclide [42].
Although the relatively small sample size of this study is a potential limitation, this study provided sufficient pilot feasibility data on the optimal imaging time point, radiation dosimetry analysis, biodistribution pattern, and, most importantly, safety of this novel tracer. Moreover, recent advances in targeted radionuclide therapy for HER2-overexpressing tumors using radiolabeled sdAbs displayed impressive results [43, 44]. This sdAb is planned to be studied in larger clinical trials for non-invasive detection of HER2 expression and targeted radionuclide therapy in breast cancer [45, 46].
{kind=link}