Study population and design
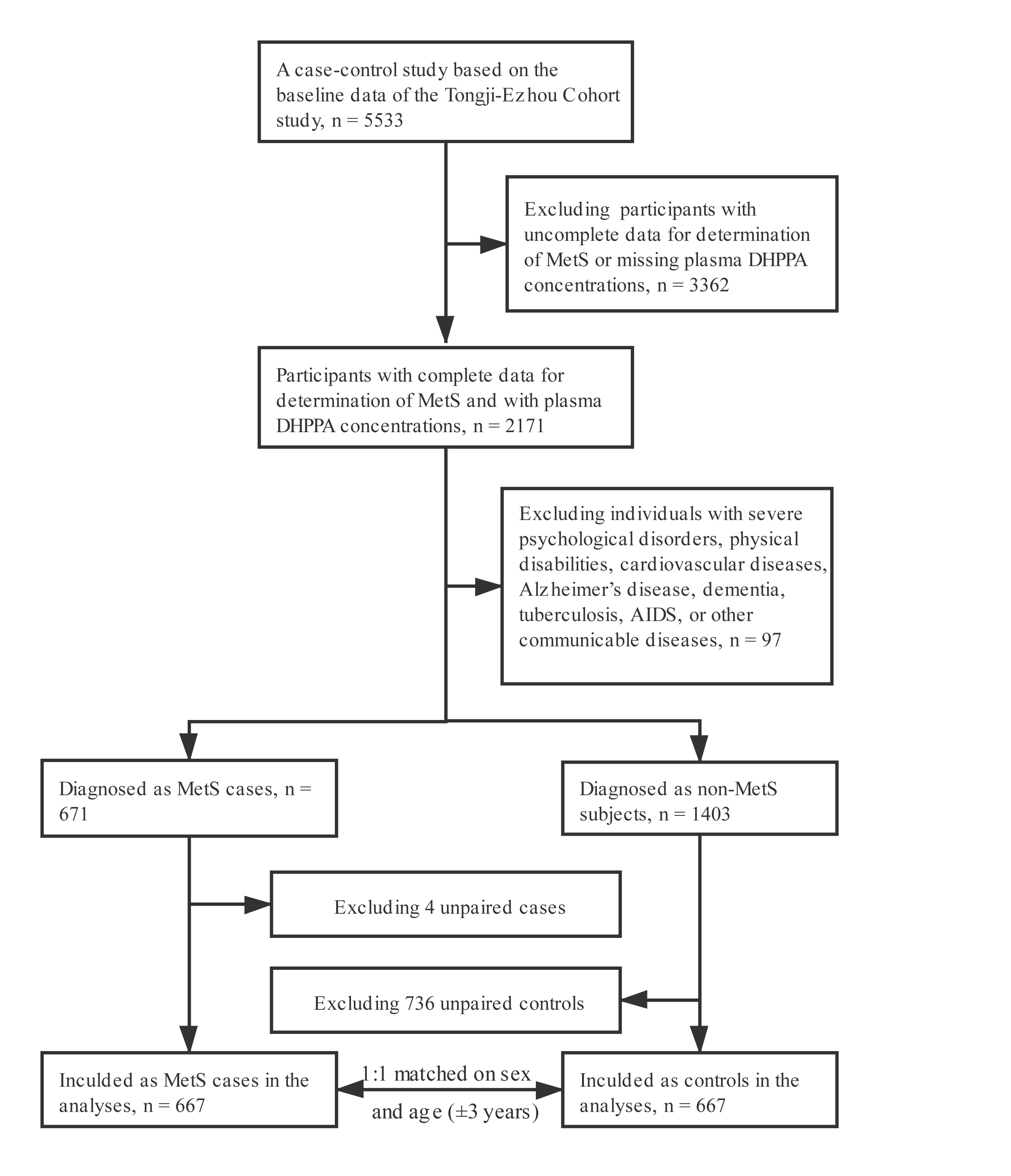
The TJEZ cohort study is an ongoing prospective cohort study investigating the associations of lifestyle, dietary factors, and genetic markers with chronic diseases. The study was set in Echeng Steel, the largest construction steel production base in Hubei Province, China. All working employees and retired employees from Echeng steel were invited to participate. Participants who were permanent residence in Ezhou and aged above 20 years at the time of recruitment were recruited. Individuals were not recruited if they had cancer or were pregnant. Between 2013 and 2014, 5533 adult residents were recruited, with a response rate of 96.6%. Data allowing the determination of the status of MetS was available for 4137 of the baseline individuals, and the prevalence of MetS was 33.6%. Among them, we excluded 1966 individuals without plasma DHPPA data, and 97 individuals with severe psychological disorders, physical disabilities, cardiovascular disease, Alzheimer’s disease, dementia, tuberculosis, AIDS, or other communicable diseases. Finally, 667 members classified as MetS were included in the analyses. Each MetS case was matched with 1 control individual. Control individuals were randomly selected among participants without MetS in the TJEZ study at baseline, and matching variables including sex and age (±3 years). The flow chart of participant recruitment and case-control selection is shown in Additional file 1: Figure S1. Ethics approval was granted by the Ethics and Human Subject Committee of Tongji Medical College. All enrolled participants gave written informed consent.
Data collection
Demographic characteristics and medical history were collected at baseline using standardized, self-administered questionnaires. Lifestyle factors including smoking habits, alcohol drinking status, and physical activity were also obtained via questionnaires. Individuals who reported smoking ≥ 1 cigarette/day over the past 6 months were considered as smokers, otherwise, they were defined as nonsmokers. Alcohol drinking status was classified as current drinking (≥ 1 time/week over the previous 6 months) and nondrinking. Physical activity was defined as regular exercise for at least 60 min per week over the previous 6 months. Education level was grouped into three categories: none or elementary school, middle school, and high school or college. Physical examinations including anthropometric measurements were performed by trained nurses. Body weight and standing height were measured in light indoor clothing and without shoes. Waist circumference were measured at the narrowest level over light clothing, using an upstretched tape meter, and measurements were recorded to the nearest 0.1 cm. Body mass index (BMI) was calculated by dividing the weight in kilograms by the square of the height in meters. Resting blood pressure were measured in a seated position after 5 minutes of seated rest. A standard mercury sphygmomanometer was used for obtaining measurements.
After overnight fasting, venous blood samples were collected from all participants at enrollment. All samples were separated for plasma within 1 hour and stored in -80℃ freezers until laboratory analysis. Fasting plasma triglycerides, total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and glucose were obtained with automated bioassays.
MetS case definition
MetS was characterized according to the harmonized criteria as the presence of at least three of the following risk factors (24): (1) central obesity: waist circumference ≥ 90 cm in men or ≥ 80 cm in women (following Chinese-specific cutoffs for abdominal obesity defined by the International Diabetes Federation) (25); (2) Hypertriglyceridemia: triglycerides ≥ 1.70 mmol/L; (3) Low levels of HDL-C: HDL-C < 1.03 mmol/L in men or < 1.30 mmol/L in women; (4) High blood pressure: blood pressure ≥ 130/85 mmHg or use of antihypertensive medication; (5) High fasting glucose: ≥ 5.56 mmol/L or current use of antidiabetic medication or self-reported history of diabetes.
Measurement of plasma DHPPA concentrations
Plasma DHPPA was measured by high-performance liquid chromatography-tandem mass spectroscopy (LC-MS/MS) (AB Sciex QTRAP 4500, Applied Biosystems, Foster City, CA). Samples from cases and controls were randomly assayed. Prior to analysis, all samples were thawed, mixed thoroughly by vortex. Then, 50 μL of plasma sample was spiked with the internal standard (1 ng of syringic acid). The sample was hydrolyzed overnight at 37℃ with β-glucuronidase/sulfatase and then extracted with acetonitrile. After centrifugation, we collected the supernatant and repeated the procedure once. The combined supernatants were evaporated to dryness under vacuum at 35℃ and reconstituted with 50 μL solvent (acetonitrile/water, 1:1, vol/vol). After centrifugation 20,238 ´ g at 4℃ for 5 min, 5 μL of the supernatant was analyzed with LC-MS/MS. Four replicate quality control samples were analyzed in each batch (n = 48). Both the intra- and interassay coefficients of variation were < 10%.
Statistical analysis
General characteristics were presented as means ± standard deviations for parametrically distributed variables, medians (interquartile ranges) for nonparametrically distributed variables, and percentage for categorical variables. Differences in descriptive characteristics between the case and control groups were explored using Student t test (normal distribution) or Mann-Whitney U test (non-normal distribution) for continuous variables; for categorical variables, the chi-square test was used. Plasma DHPPA concentrations were considered as continuous variable and categorized into quartiles according to their distribution among the controls (quartile 1, < 7.74 nmol/L, quartile 2, 7.75-12.30 nmol/L, quartile 3, 12.31-20.97 nmol/L, quartile 4, ≥ 20.98 nmol/L). Logistic regression models were used to estimate odds ratios (ORs) and 95% standard deviations (CIs) of MetS in relation to plasma DHPPA concentrations. The regression models were adjusted for age, sex, BMI, current smoking, current alcohol drinking, physical activity and education level. Linear trend P-values were estimated by modeling the median value of each plasma DHPPA category as a continuous variable. To further examined the the potential nonlinear relation between plasma DHPPA and MetS, we used a cubic spline regression model with 4 knots at the 20th, 40th, 60th, and 80th percentiles of plasma DHPPA concentrations.
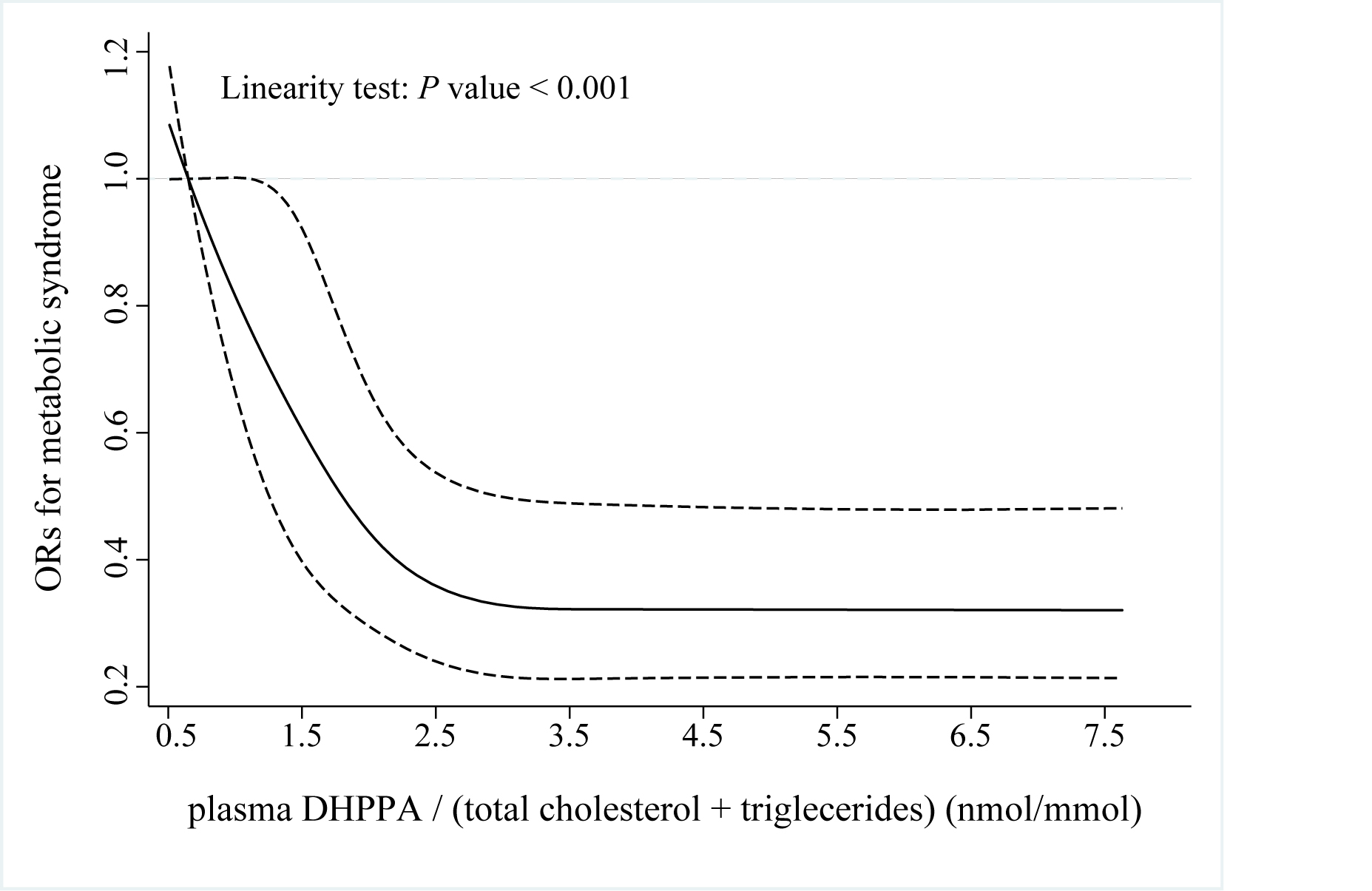
Given that plasma alkylresorcinols-precursor of DHPPA-are transported in lipoprotein (16), the variations in carrier lipoprotein concentrations might result in their difference in plasma DHPPA concentrations. Hence, a new variable-plasma DHPPA / (total cholesterol + triglycerides) index-was generated to adjust for variations in the concentrations of carrier lipoproteins. Similar to plasma DHPPA concentrations, plasma DHPPA / (total cholesterol + triglycerides) index was considered as a continuous variable and categorized into quartiles according to its distribution among the controls (quartile 1, < 1.27 nmol/mmol, quartile 2, 1.28-2.14 nmol/mmol, quartile 3, 2.15-3.62 nmol/mmol, quartile 4, ≥ 3.63 nmol/mmol). Logistic regression models were fit to estimate odds ratios (ORs) and 95% standard deviations (CIs) of MetS in relation to plasma DHPPA / (total cholesterol + triglycerides). The regression models were adjusted for age, sex, BMI, current smoking status, current alcohol drinking status, physical activity and education level. Linear trend P-values were estimated by modeling the median value of each plasma DHPPA / (total cholesterol + triglycerides) category as a continuous variable. To further examined the potential nonlinear relation between plasma DHPPA / (total cholesterol + triglycerides) and MetS, we used a cubic spline regression model with 4 knots at the 20th, 40th, 60th, and 80th percentiles of plasma DHPPA / (total cholesterol + triglycerides) index.
To estimate the consistency of the DHPPA-MetS association according to participant characteristics, we conducted stratified analyses by sex, age (<50 and ≥50 years), BMI (<24 and ≥24 kg/m2), current smoking status (yes or no), current drinking status (yes or no) and physical activity (yes or no). Interactions between plasma DHPPA categories and these confounding factors on ORs of MetS were tested using likelihood ratio tests, comparing models with and without multiplicative interaction terms. Statistical analyses were performed with SPSS 23.0 software (SPSS, Inc.) and Stata/SE 12.0 software (StataCorp LP). P < 0.05 was considered significant.
{kind=link}
{kind=link}