Interpretation and comparison with the literature
Intracranial hemorrhage is a significant and feared complication of ECMO therapy. Its incidence is reported to be between 2 9 and 10% 10,11. Some authors report rates as high as 25% 12, but this is probably related to the fact that these studies include patients with venoarterial ECMO. The occurrence of intracranial hemorrhage has a high impact on prognosis 11,13,14 with up to 74% mortality at one month in these patients 15. It could also impact cognitive outcome 16. It should also be stressed that the exact incidence of intracranial hemorrhage under ECMO is difficult to assess since it is not always possible and potentially dangerous to perform a head CT scan before or during ECMO therapy. Moreover, it is sometimes difficult to establish that neurological complication is posterior to the onset of ECMO treatment. One recent study 13 in which investigators performed a routine head CT scan within 24hours of cannulation showed that 10% of patients presented an intracranial hemorrhage. While SARS-CoV-2 infection could be associated with the occurrence of spontaneous intracranial hemorrhage 2 (in patients not treated with ECMO), it is unknown whether there is an increased risk of intracranial hemorrhage in SARS-CoV-2 infected patients treated with ECMO as compared to non-SARS-CoV-2 patients treated with ECMO. A recent study 17 reported a 41.7% incidence rate in a series of 12 patients infected with SARS-CoV-2. This contrasts with another recent study that found a 5% incidence in a series of 83 patients with COVID-19 treated with ECMO 1.
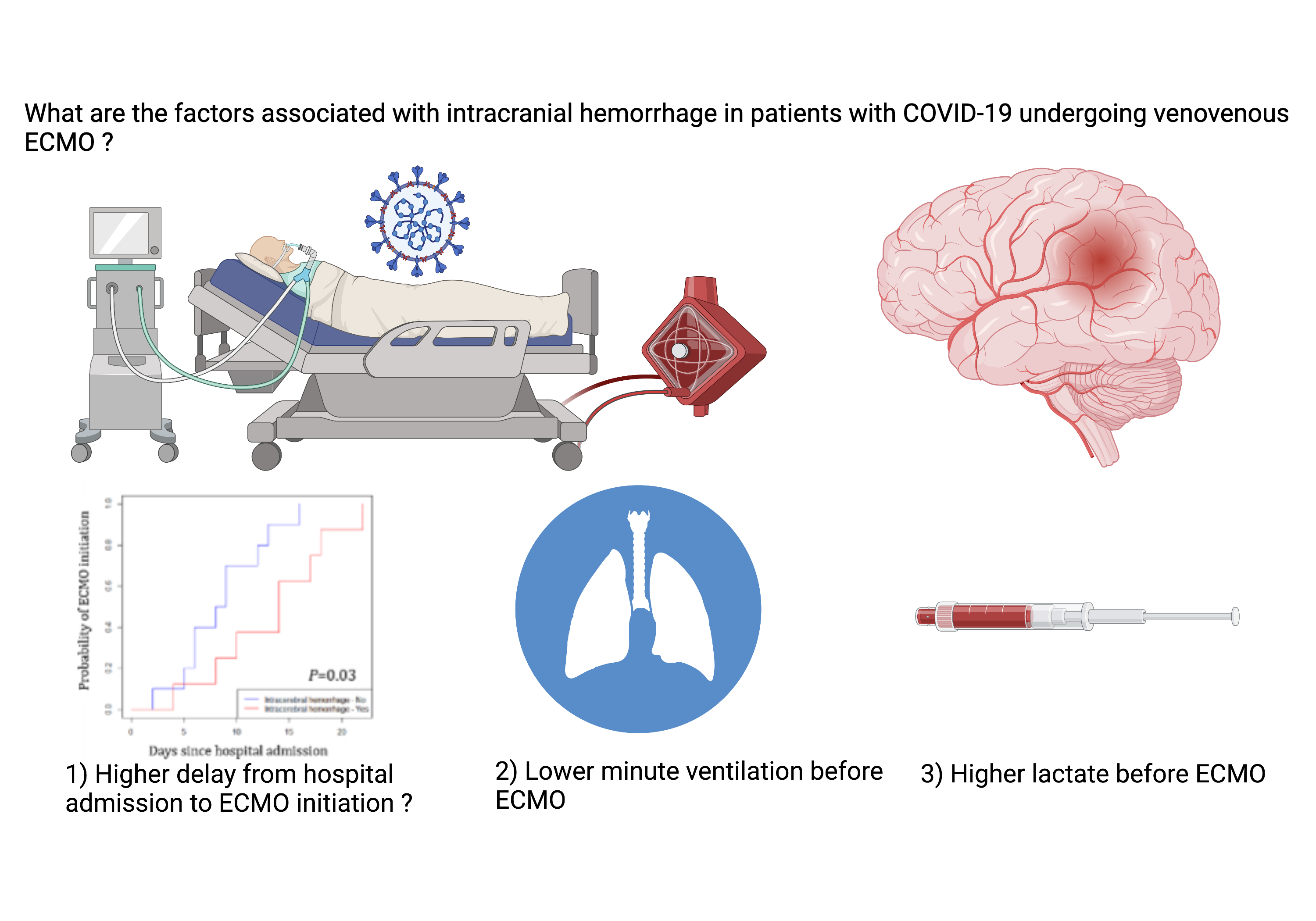
The main result from our study is the association between intracranial hemorrhage and a longer delay between hospitalization and ECMO initiation. Although this result has to be confirmed by future studies, we believe it is highly relevant for clinical practice, since it could inform the decision of initiating ECMO in patients with COVID-19. Intracranial hemorrhage tended to occur early after ECMO onset. As a result, duration of ICU stay and mechanical ventilation was shorter in patients with intracranial hemorrhage. Therefore, the association between later onset of ECMO and intracranial hemorrhage does not seem to be mediated by a longer period of ECMO therapy. Contrary to a previous study 18 intracranial hemorrhage was not associated with the delay between intubation and ECMO onset.
The type of intracranial hemorrhages observed in our study is in accordance with the literature. Intraparenchymal hemorrhage is the most frequently reported complication 6,13, followed by subarachnoid hemorrhage 6,9,18. CT Fluid-Blood levels are considered specific for the presence of coagulopathy 19 and have already been described in the setting of ECMO for SARS-CoV-2 infection 20. In our series, five out of eight patients with intracranial hemorrhage presented a nasal fossa hematoma which further supports the implication of hemostasis disorders in intracranial hemorrhage observed in this study. In comparison with previous studies 9,21, we did not include patients with microbleeds in the intracranial hemorrhage group. Microbleeds have been described 22 on MRI in patients who survive ECMO and do not seem to be associated with a poor neurological prognosis. Besides, they might not be specific to ECMO therapy as they have been described in patients surviving sepsis (SARS-CoV-2 related 23 and non-SARS-CoV-2 related 24).
In the literature, factors associated with the occurrence of an intracranial hemorrhage include hematosis and mechanical ventilation parameters (rapid correction of hypercapnia 9), hemostasis 6,13,18, liver function 14, kidney function 9,13, renal replacement therapy 6,14, circulatory dysfunction and cardiac arrest 11,14.
We found that hypoventilation was associated with the occurrence of intracranial hemorrhage. A previous study found an association between intracranial hemorrhage and rapid correction of hypercapnia 9, which might relate to the same physiological phenomenon. Hypercapnia is responsible for cerebral hyperperfusion 25 and has been proposed as a risk factor for intraventricular hemorrhage in preterm infants 26. However, this last point is disputable 27 and intraventricular hemorrhage in this population might rather be related to rapid variations in capnia 28. Importantly in our cohort of 42 patients, there was no correlation between time from hospitalization to ECMO and minute ventilation before ECMO initiation. This suggests that our results in the 18 patients showing decreased minute ventilation and longer delay for ECMO initiation in patients with intracranial hemorrhage are independent and might correspond to different biological phenomena.
In accordance with literature 11,14 we found an association between circulatory dysfunction (higher arterial lactate) and intracranial hemorrhage. We also found a tendency for higher bilirubin in the intracranial hemorrhage group, which is consistent with the literature 14.
In our series all but one patients with intracranial hemorrhage died. While two of them fulfilled the criteria for brain death, it should be acknowledged that the neurological prognosis was more uncertain for other patients. Managing these patients represents a clinical and ethical challenge. Fletcher-Sandersjöö et al. 15 reported on 38 patients in which the diagnosis of intracranial hemorrhage under ECMO did not result in limitation of life-sustaining therapies. For 12 patients, the hemorrhage was considered of no clinical significance and did not result in a new intervention. In 26 patients, the diagnosis of intracranial hemorrhage prompted a modification of treatment. Management included the correction of hemostasis disorders (n = 19), decannulation (n = 9), medical management aiming at controlling intracranial pressure (n = 14), and neurosurgery (n = 5). Among these 38 patients, 17 of these patients survived, and among them ten (59%) had a favorable neurological outcome six months after ICU.
Limitations of our study
Our study's major limitation is its small size, which is probably responsible for a lack of statistical power. This limited our ability to perform a multivariable statistical analysis. The monocentric and retrospective design limits the generalizability of our results.
Another major limitation of our study is the lack of data regarding the anticoagulation regimen and coagulation tests in our patients. It is very likely that the occurrence of intracranial hemorrhage is related to the anticoagulation regimen. In our study there was a tendency for a higher rate of severe bleeding requiring transfusion in patients with intracranial hemorrhage. The multiloculated and compartmentalized aspect with fluid-fluid levels observed in our patients has been shown to be specific for the presence of a coagulopathy 29.
We were also not able to study the effect of COVID-19 on the risk of intracranial hemorrhage under ECMO, as we didn’t include patients without COVID-19.
Our study might also suffer from the fact that head CT is not routinely performed in patients treated with ECMO. This has obvious clinical reasons since the transportation of these patients to the CT scan bears risks for the patient and is time and resource-intensive. As a consequence, it is possible that intracranial hemorrhage might have been undiagnosed in some patients, including the most severe patients who could not be transported to the CT scan. Pupillary abnormalities or disturbed transcranial Doppler values were present in most patients diagnosed with intracranial hemorrhage in our series. However, they were not specific as three patients with pupillary abnormalities/pathological transcranial Doppler had no signs of intracranial hemorrhage on CT scan. This seems also to be the case for epilepsy, although our sample is too small to draw any conclusion.
{kind=link}