The 62-year-old female patient was admitted to neurology emergency at 8:50 am on November 1st, 2019, due to "sudden verbal slant accompanied by left limb weakness for 1.5 hours".She was suddenly appeared the left side of the mouth aslant, conscious of numbness and weakness of the limb on the same side, when she was having breakfast in the morning (7:20 am), and could still walk by herself without headache, dizziness, unclear vision, speech deficit or any other manifestations.Her family drove her to the hospital immediately.She had a history of hypertension for more than 30 years without regularly monitoring. The highest blood pressure was 150/100 mmHg, taingvalsartan 80mg Qd. She also had a hyperlipidemia history for 6 years, with long-term administrationrosuvastatin 5mg Qn.She was hospitalized in our department of cardiology 6 months ago due to "atrial flutter" and received betaloc 12.5mg twice daily. One month ago she was hospitalized again in another hospital and diagnosed as "pathological sinus syndrome and paroxysmal atrial fibrillation" due to "atrial fibrillation", and was treated with dabigatran 110mg twice daily but without a good compliance. She had no specialfamilyhistory, or history of migraine. Physical examination: BP: 131/81mmhg (right) 130/84mmhg (left).There was no uplift or depression in the anterior cardiac area, and the strongest apex pulsation point was 0.5-1.0 cm within the midline of the 5th intercostal left clavicle. There was no lifting pulsation, no tremor or pericardial friction.The relative voiced boundary of the heart is normal.Heart rate: 76 beats/min, regular rhythm, normal cardiac sounds, A2 >P2, no extra cardiac sounds, no cardiac murmurs, no pericardial fricative sounds in the auscultation area of each valve.
The patient had clear mind and fluent speech, equal circle of bilateral pupils, direct/indirect response to light exists, and the eyeball moves fully in each direction, without diplopia and nystagmus. The left frontal line, nasolabial groove shallow, show the mouth angle to the right, extending tongue in the center.Double soft palate lift normal, uvula in the middle, pharyngeal reflex normal. Muscle strength of left limb grade V-, bilateral finger nose test and heel-knee-tibia test accurate, bilateral Babinski’s sigh negtive.Hypoesthesia of left limb, Meningeal stimulation negtive.Water swallow test normal.Bilateral carotid artery vascular murmur were not heard.NIHSS score: 4 (2 for facial paralysis, left weakness 1, left Numbness 1).
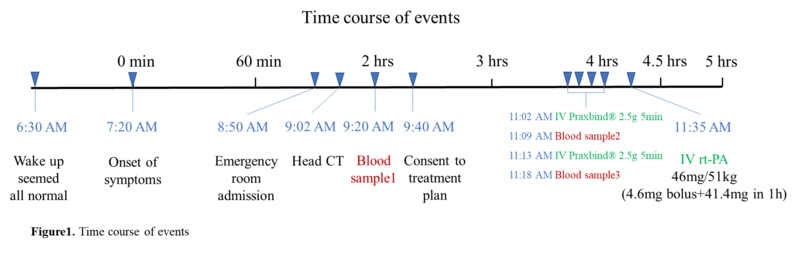
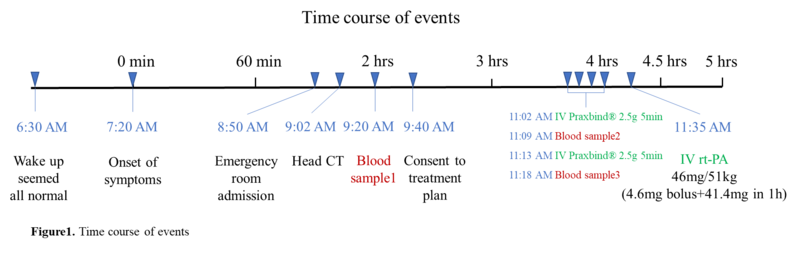
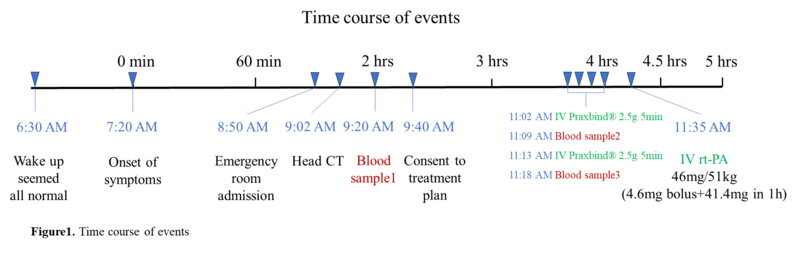
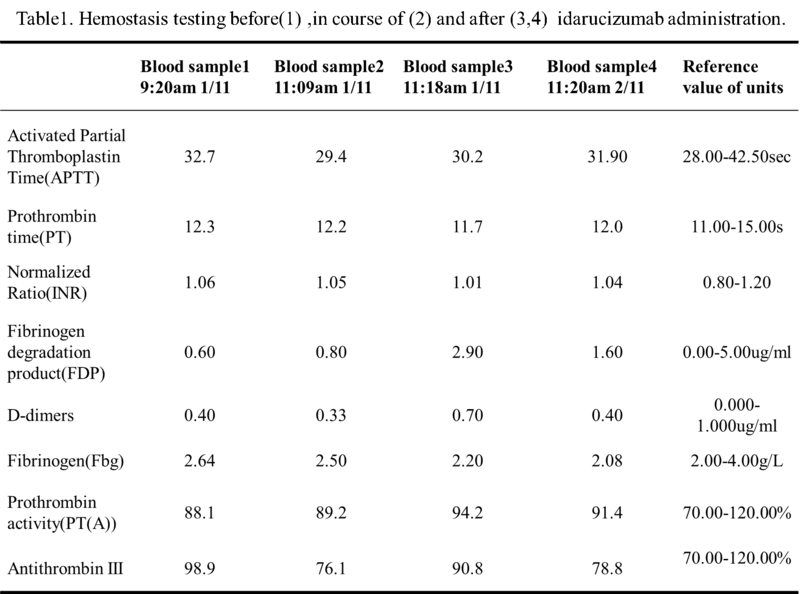
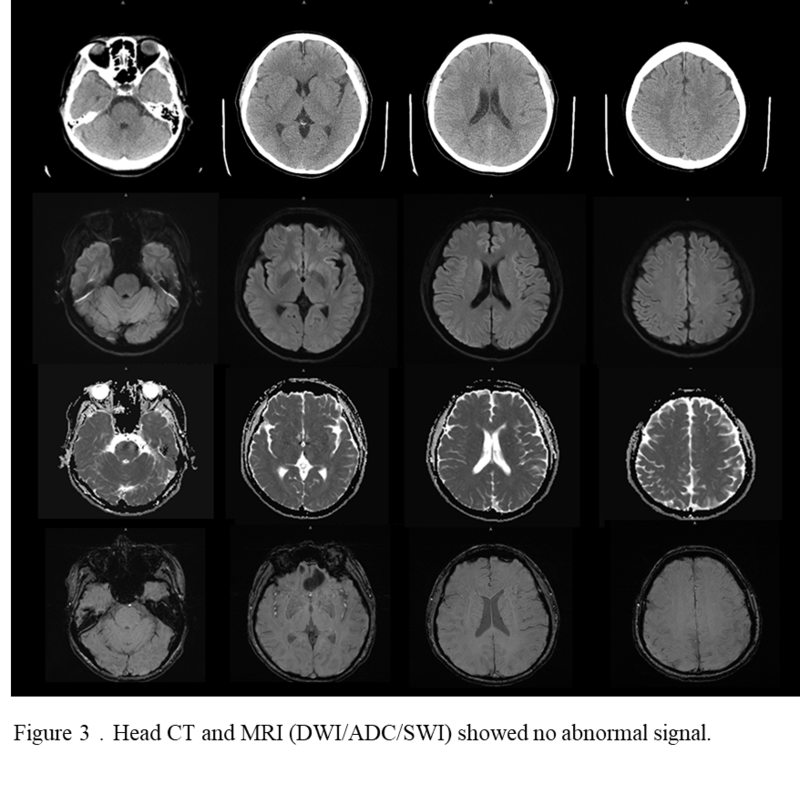
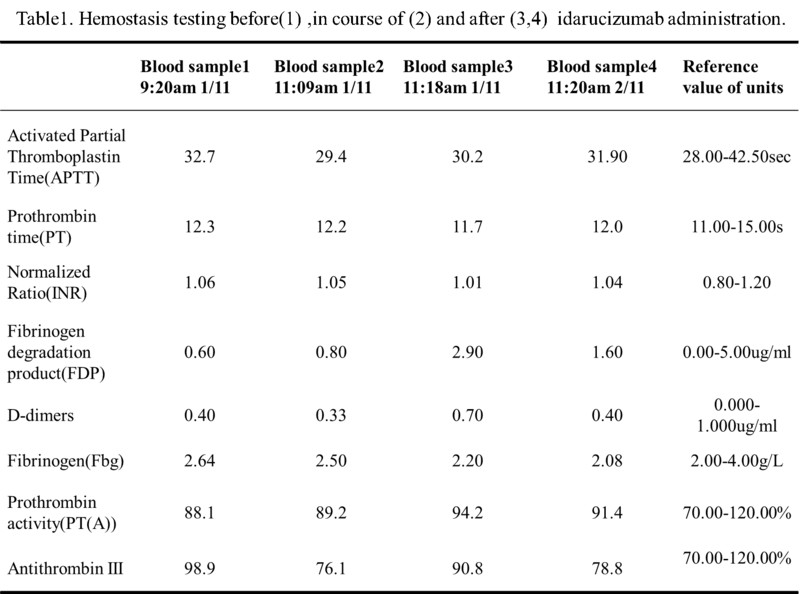
The patient mentioned that she did notve take any drugs in the morning and that she missed one dose of dabigatran last night. The last time for taking dabigatran was around 8am the day before. Accordingly, the last DOAC dose taking was between 24-48 hours.Then she had been brought into the emergency fast track for stroke, completed head CT, ECG, blood routine, biochemical and coagulation function test.Her head CT was normal, blood glucose was 5.5mmol/L, and the ECG showed sinus rhythm of 72 beats/min. Coagulation function results showed APTT 32.7s, PT 12.3s, INR 1.06, CCr 68.62ml/min.AS ECT and direct prothrombin activity could not be tested, idarucizumab was be given at 11:02 am with a dose of 2.5 g, followed by another 2.5 g at an interval of 5 minutes, and coagulation function was be tested again after the administration (Table 1). The rt-PA thrombolysis therapy was initiated at 11:35 am after the completion of the administration of idarucizumab, with a dose of 0.9 mg/kg. During the thrombolysis process, vital signs such as heart rate and blood pressure were monitored, and the NIHSS score was evaluated every 15 minutes (Figure 1). The symptoms of facial paralysis and limb numbness and weakness of the patient were significantly improved after thrombolysis. The NIHSS score was 1 (facial paralysis 1), and the patient was admitted to the stroke ward for further treatment.
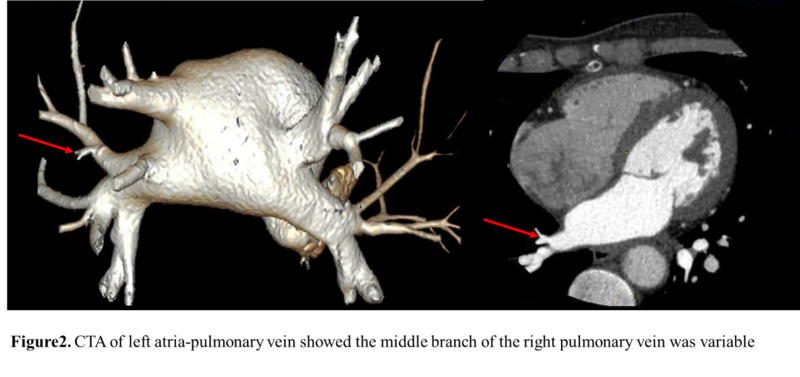
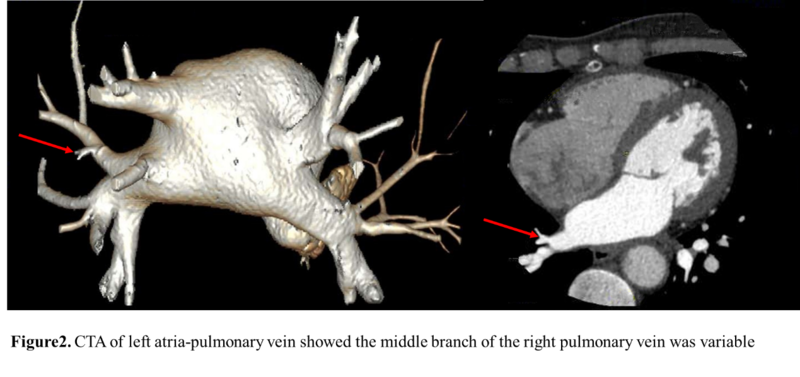
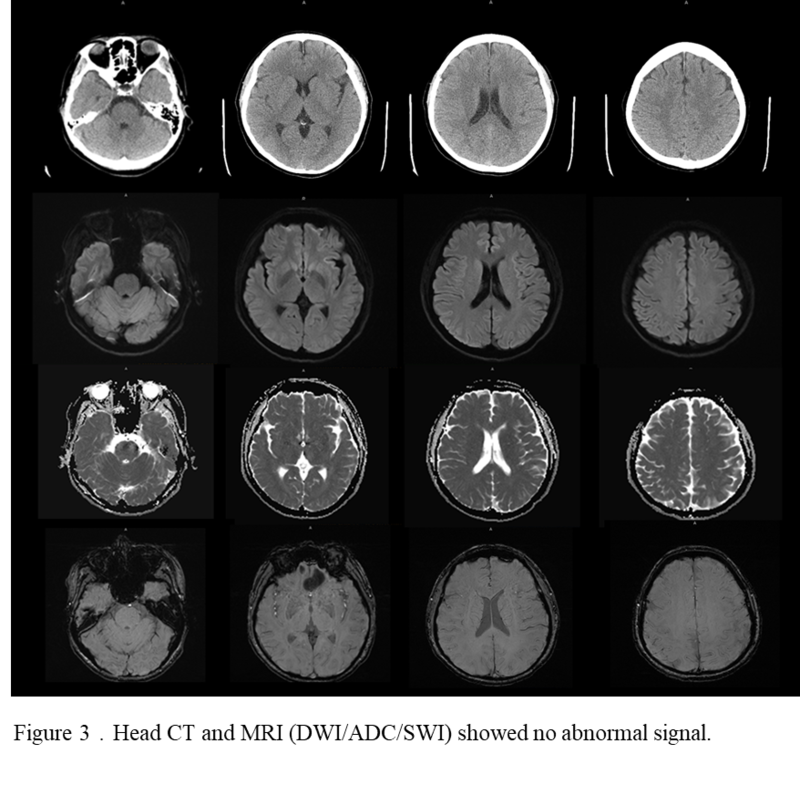
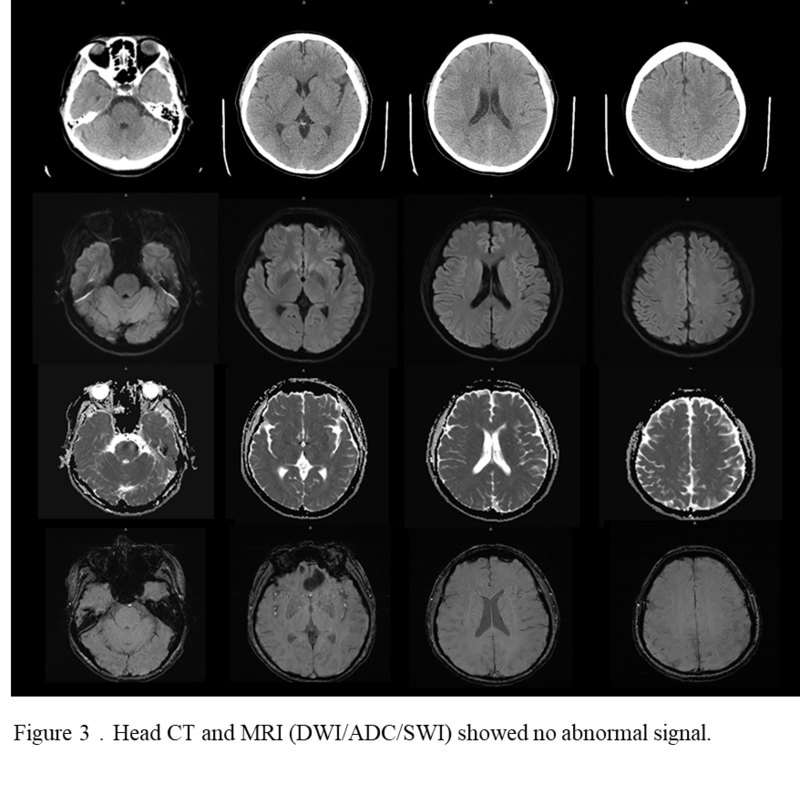
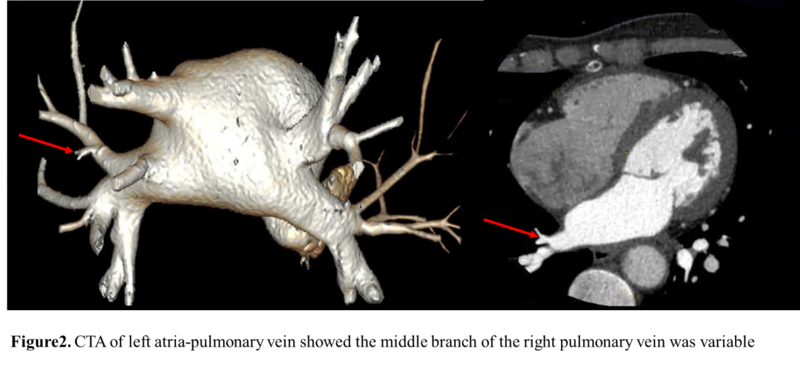
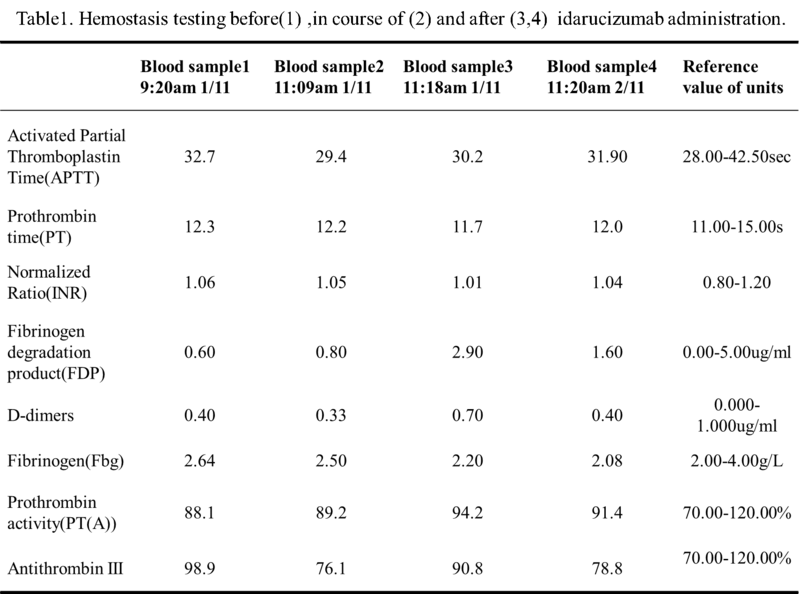
Vital signs were monitored within 24 hours after admission, the patient got external auditory canal bleeding3 hours after thrombolysis. Further more medical history was inquired, and the patient had a history of ear trauma one week ago. Bleeding was stopped by external auditory canal tamponage.The cranial MRI and systemic vascular examination were arranged to find the cause of stroke, no abnormal signal was found in T1, T2 and DWI, and no microhemorrhage was found in SWI (Figure 2).MRA showed intracranial vessels were normal, and bilateral embryonic posterior cerebral arteries were found. Carotid ultrasound showed bilateral carotid intima thickening with plaque formation and plaque was found in right subclavian artery. Arteriovenous ultrasound of lower extremity showed normal. Transcranial Doppler (TCD) showed a rapid increase in the flow rate of the left middle cerebral artery, and 5-6 microembolic could be found in foaming experiment which indicated there may be direct pathway from pulmonary circulation to systemic circulation (RLS). Cardiac systemic examination was completed: 24-hour Holter showed sinus bradycardia, short atrial tachycardia, and atrial premature beats (some of which were not transmitted). Widening ascending aorta was showed on echocardiography.No thrombus was found in Bilateral atrium and left aurcle through Transesophageal echocardiography,also no septal shunt beam was observed in the atrial septal fossa ovale. A further review of the data in other hospital before showed left atrium was slightly larger and the middle branch of the right pulmonary vein was mutated on the CTA of the left atria and pulmonary veins at 26thSeptember (Figure 3). Diagnosis of transient ischemic attack (TIA), cardiogenic cerebral embolism, paroxysmal atrial fibrillation, pulmonary arteriovenous fistula,hypertension (Grade 2), and hyperlipidemia were made after admission. She was suggested to restart the anticoagulant treatment deal to the CHA2DS2-VAS score was 4 and HAS-BLED score was 2. The pulmonary artery DSA was also be suggestedafterdischarged.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}