Study population
A prospective, observational, single-center study of consecutive patients admitted to our institution for confirmed COVID-19 pneumonia since 31 March 2020 to 5 May 2020 was conducted. We included patients with a positive COVID-19 nasopharyngeal polymerase chain reaction (PCR) receiving at least one dose of one of the following QTc-prolonging drugs: azithromycin (AZ), hydroxychloroquine and/or lopinavir-ritonavir. Patients in which a baseline ECG and at least one follow-up ECG during active treatment were not carried out were excluded for the analysis (Figure 1).
In order to safely confirmed feasibility of QTc measurement with KardiaMobile-6L compared to conventional 12-lead ECG, both registries were sequentially obtained in a consecutive cohort of healthy patients with negative COVID-19 PCR as a control group.
Study procedures
MEDICAL TREATMENT
The choice of treatment in each patient was based on physician´s criteria and local guidelines. Changes in medication, including those related to iatrogenic QTc prolongation, were individualized.
ELECTROCARDIOGRAPHIC MONITORING
As proposed by Giudicessi et al., an ECG was performed in all patients receiving at least one QTc-prolonging medication before any drug was started and repeated at 48 hours and 96 hours, and every 2-3 days while continuing any of these therapies(3). ECG recordings during admission were carried out using 12-lead conventional ECG or KardiaMobile-6L device depending on its availability (the smart device was progressively implemented in daily practice) and the clinical condition of the patient (since 6-lead ECG with the handheld device could only be obtained in relatively stable conscious subjects). Patients were allocated in 3 groups for the analysis depending on the device used to measure the QTc at baseline and during follow-up within the admission (Figure 1): A) conventional 12-lead ECG before and after COVID-19 therapies were started; B) conventional 12-lead ECG at admission, followed up with handheld device; and C) fully monitored with heart rhythm smart device. If both ECG devices were used in the same patient during follow-up, only the recording with the longest QTc was taken into account.
Conventional 12-lead ECG was obtained as in common clinical practice, although the equipment needed to be fully cleaned and disinfected before leaving the room afterwards. To register a 6-lead ECG with the handheld device, the patient was told to be sit and place the device on the bare skin of his left leg (at the knee or the ankle) holding his thumbs on the top of two electrodes for 30 seconds (Figure 2A). If the patient could not sit, the ECG was recorded while lying down, flexing the left knee closer to the body (Figure 2B). Alternatively, 1-lead ECG (lead I) could be obtained only with two fingers in contact with the electrodes. The ECG registry was wirelessly transmitted to a tablet outside the patient’s room and digitally uploaded by a dedicated app to a secure server. Once the device was used, the electrodes were cleaned spraying with an alcohol-based sanitizer and wiping with a soft cloth before being used in another patient. Since ECG recording with the handheld device requires the active collaboration of the patient, standard 12-lead ECG was carried out among those in worse clinical status. Similarly, if an accurate registry could not be obtained for whatever reason, a conventional 12-lead ECG was performed.
In order to assess healthcare workers exposure, the duration of the ECG recording was documented for each ECG registry (when possible) and compared between both techniques. Procedural time accounted since the healthcare worker entered into the patient’s room to the disinfection of the device (either conventional 12-lead ECG or KardiaMobile-6L) once the register was performed. Similarly, ECG recording time was addressed in the healthy control cohort (since the patient lied down in bed until postprocedural disinfection measurements were completed).
QTc MESUREMENT
ECGs records were reviewed and interpreted by at least one of 2 trained cardiologists (C.M.C. and J.E.M). QTc interval was calculated using Bazzet’s formula in leads II or V5 in the 12-lead ECG and in lead II when using the handheld 6-lead ECG(4). If these leads did not provide an accurate end of the T wave, I and aVL were preferably used as an alternative, although QTc measurement in any other lead was permitted. For patients with a wide QRS from either ventricular pacing or left/right bundle branch block the excess correction method was used(5). In patients with atrial fibrillation (AF), QTc was estimated as the mean of 3-5 beats. To ensure the integrity of the data, none of the ECG interpreters knew the therapy administered to the patient.
The longest QTc measured after COVID-19 drugs were started was considered as peak QTc during admission and compared with the QTc at baseline to evaluate QTc prolongation. Patients with a peak QTc ≥ 500ms and those with an increase in the QTc ≥ 60ms from baseline values were considered at high risk for VA(6).
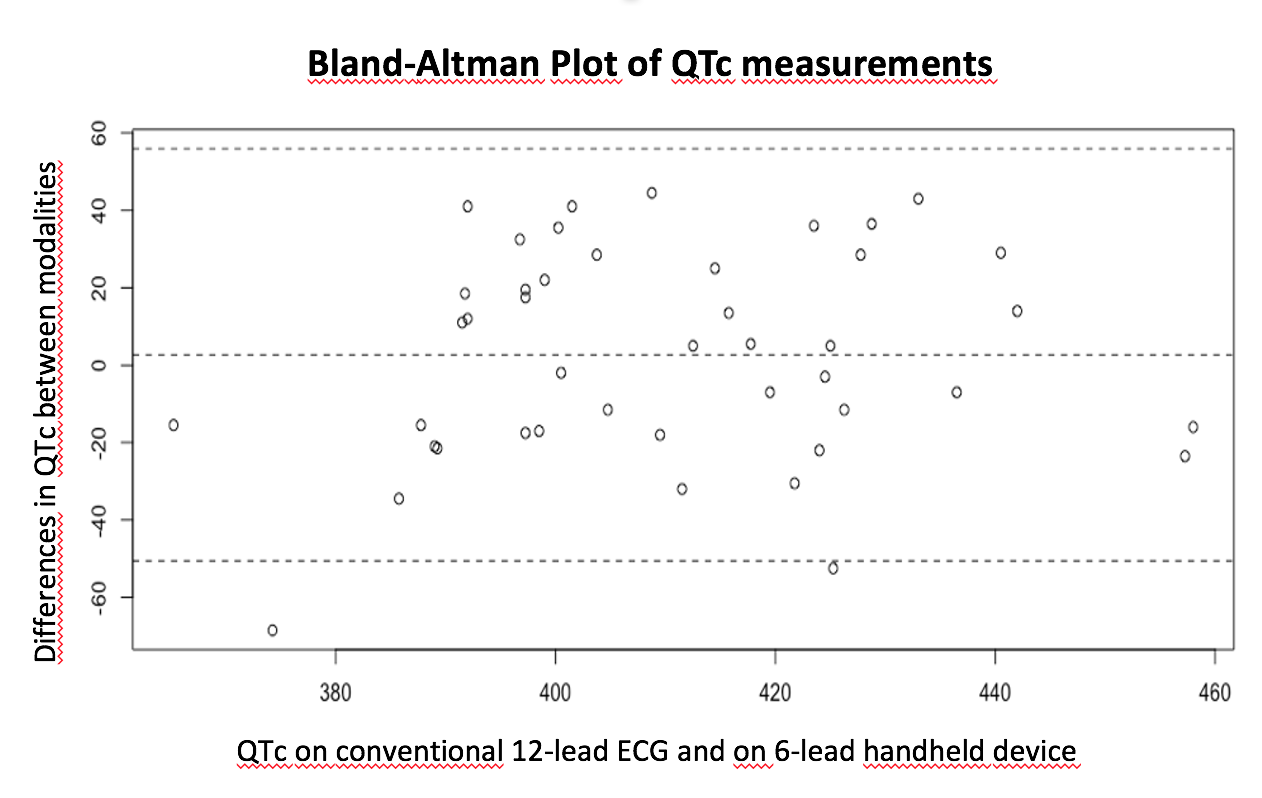
With the aim to evaluate the feasibility of QTc measurement with 6-lead handheld device compared to conventional 12-lead ECG, QTc was also blindly address in the healthy control cohort.
Study endpoints
The main objective of this study was to evaluate differences in QTc monitoring in COVID-19 patients receiving QTc-prolonging drugs between conventional 12-lead ECG and 6-lead heart rhythm handheld device. Time needed to obtain an ECG registry with both devices was set up as a secondary endpoint.
Data collection
All data were collected using standardized report forms including demographic features, medical history, baseline clinical characteristics, biochemical and ECG findings, medical treatment during admission and in-hospital clinical outcomes. CURB65 (Confusion, BUN >19 mg/dl, Respiratory rate < 30, Systolic blood pressure < 90 mmHg or diastolic blood pressure<60 mmHg, Age > 65 years) and Tisdale scores were estimated at admission. Clinical follow-up was carried out during hospitalization addressing all-cause mortality. The study was approved by the local Ethics Committee and adhered to the principles outlined in the Declaration of Helsinki. Individual informed consent was obtained from participants.
Statistical analysis
Continuous variables were summarized as mean ± standard deviation (SD) or as medians and interquartile range (IQR) and were compared between groups using ANOVA or Kruskall Wallis tests depending on normality. Differences in the time of ECG recording between devices and changes in QTc from baseline to peak were compared using paired or unpaired Student T tests or the non-parametric Wilcoxon rank sum tests if the normal distribution the variables could not be demonstrated. Categorical variables were described as percentages and compared using Chi-square or Fisher exact tests according to expected frequency over or below 5, respectively. Derangement from the normal distribution was assessed with the Shapiro-Wilk test. A two-sided p-value < 0.05 was regarded as statistically significant. Statistical analyses were performed using STATA software version 15.1.
{kind=link}