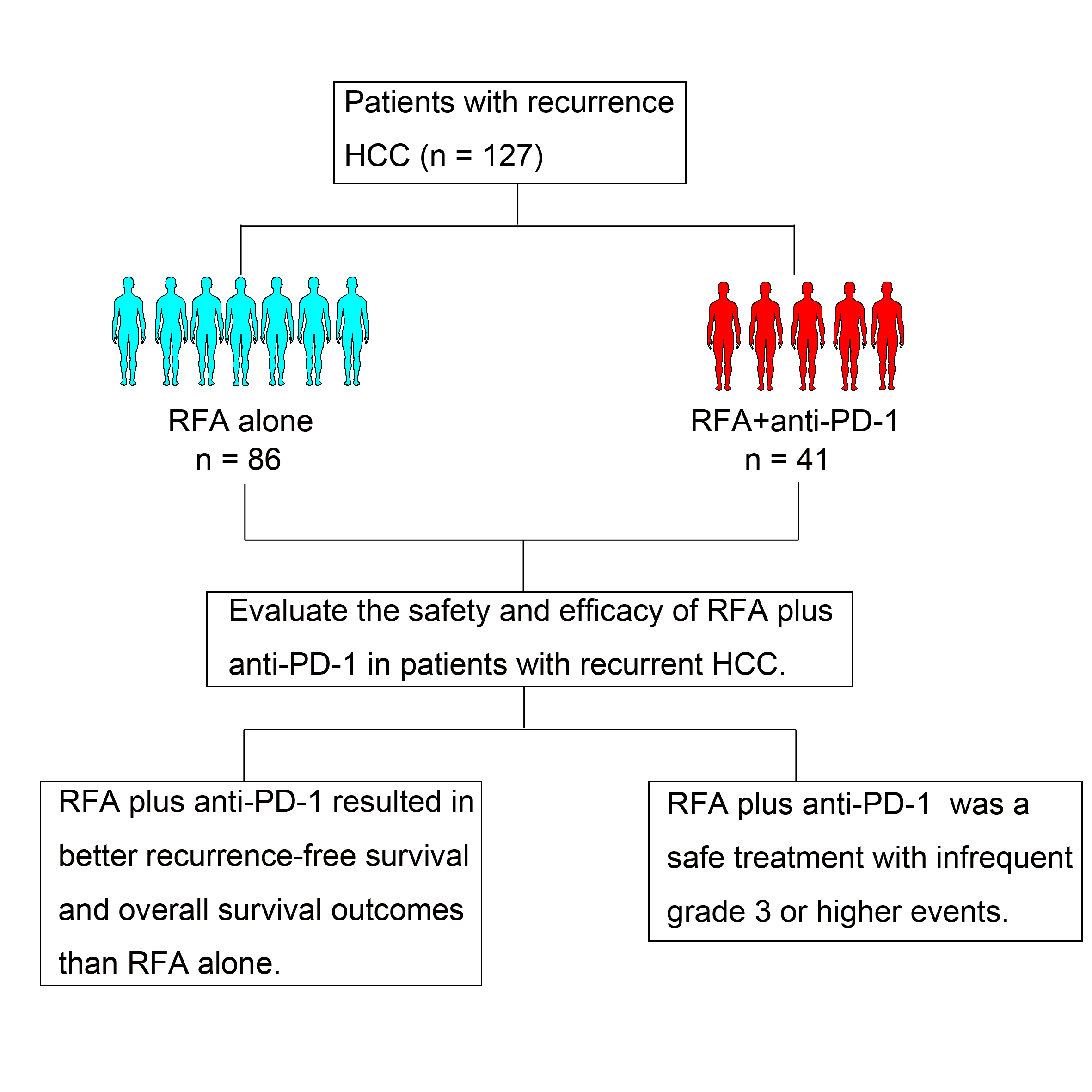
In this retrospective study, we firstly reported the efficacy of anti-PD-1 therapy on RFS and OS outcome in recurrent HCC after curative RFA treatment. Our results showed that patients with recurrent HCC had significant better RFS and OS outcome in the RFA + anti-PD-1 group than in the RFA alone group.
Previous studies showed that single-agent checkpoint inhibitors did not show a better survival outcome in patients with HCC (26, 27). In this study, there were two important differences with the previous reports. First, all patients enrolled in this study underwent curative RFA treatment before anti-PD-1 therapy. It has been shown that RFA induced T cell immune responses as well as PD-L1 expression in synchronous colorectal cancer liver metastases and tumor-bearing mice (22, 28). In addition, T cell immune responses induced by RFA led to a detectable antitumor reactivity in mouse models (22, 29). Previous researches showed that PD-L1 as well as PD-1 and CTLA-4 contributed to the inhibition of thermal ablation-induced antitumor activities (22, 30). Positive PD-L1 expression in patients was associated with an objective response for anti-PD-1 therapy (31, 32). PD-L1 immunohistochemistry tests for calculating the efficacy of anti-PD-(L)1 therapy in NSCLC and several other cancers has been approved by the US Food and Drug Administration (33). Thus, RFA can provide a useful antigen source for the induction of antitumor immunity. Meanwhile, some preclinical studies have shown that combining of radiotherapy and PD-L1/PD-1 blockade synergistically enhance antitumor immunity (34, 35). These results suggested that local antitumor treatments by radiotherapy can elicit immune response, thereby providing a better opportunity for PD-1/PD-L1 blockade therapy. Second, patients with BCLC stage A, no extrahepatic metastases and no invasion of the portal vein, the hepatic vein trunk or secondary branches were enrolled in this study. However, all the studies about single-agent checkpoint inhibitors treatment evaluated patients with advanced HCC (26, 27). Thus, all patients in our study had a better physical condition compared with those in the above reports.
A previous report showed that liver metastases in patients with advanced melanoma were associated with reduced ORR and progression-free survival during anti-PD-1 therapy (36). In addition, one recent report showed that patients with an ECOG performance status of 1 or more, bone metastases, and liver metastases had a shorter 5-year OS in advanced melanoma, renal cell carcinoma, or non-small cell lung cancer (37). Therefore, these results suggest that anti-PD-(L)1 therapy will provide a better clinical benefit for patients with early HCC. Our results support this concept. Findings from the current study showed that tumor number, TNM stage and anti-PD-1 treatment were significant prognostic factors for RFS and OS, and patients with one tumor experienced better clinical benefit in RFS and OS than those with two or three tumors during anti-PD-1 therapy (RFS: HR = 0.501 vs. HR = 0.645; OS: HR = 0.025 vs. HR = 0.433). Similar results were found in patients with TNM stage I. Although some studies have failed to show a better survival outcome in patients with HCC during single-agent checkpoint inhibitors therapies, more reports and our results suggested that anti-PD-1 treatment could provide a better clinical benefit for early HCC patients pretreated with RFA.
In this study, the RFA treatment-related adverse events were pleural effusion requiring drainage and mild or moderate increase in body temperature, which is consistent with historical data in other trials (14, 23). The spectrum of adverse events observed with the anti-PD1 therapy were similar to those reported in previous studies (26, 38, 39). A total of 6 patients occurred grade 3 or higher TRAEs were excluded from this study because they met the exclusion criteria. In the analysis of complications with the anti-PD1 therapy, the above 6 patients were re-included. The frequencies of any grade TRAEs and grade 3 or higher events in this study were 70.2% (33) and 12.8% (6) respectively, which is not consistent with historical data in other trials of Pembrolizumab (any grade TRAEs: 98.2%, grade 3 or higher events:61.1%) or Atezolizumab (any grade TRAEs: 96.4%, grade 3 or higher events: 52.0%) for hepatocellular carcinoma (38, 39).The lower incidence of grade 3 or higher events in our study may be due to patients enrolled with BCLC stage A, no intrahepatic and extrahepatic metastases and no invasion of the portal vein, the hepatic vein trunk or secondary branches. The patients population enrolled in this study with a better physical condition well tolerated the toxicity caused by the anti-PD-1 therapy.
Our study as a retrospective research had several limitations. The baseline demographics were matched well between the two groups, but prospective randomized controlled trials are needed for further research. In addition, the number of patients enrolled in this study was limited (41 patients in the RFA + anti-PD-1 group vs. 86 patients in the RFA alone group). Thus, studies with a larger sample size are needed to confirm our findings. Meanwhile, the follow-up time is only one year. Therefore, patients should be followed up for assessment of RFS and OS at least 3–5 years in the future study.
In conclusion, RFA + anti-PD-1 is a safe and effective therapy for recurrent HCC patients with BCLC stage A, tumor diameters smaller than 3 cm and no more than three tumors, no extrahepatic metastases and no invasion of the portal vein, the hepatic vein trunk or secondary branches.
{kind=link}