As a suspected case of COVID-19, a 51-year-old female patient admitted to the hospital presented with the symptoms of a “cough, runny nose, and a fever for 2 days” and a maximum body temperature of 37.8℃. The family cluster included seven family members; the patient’s husband, daughter, son-in-law, son, two grandchildren. Within this group the oldest was 65 years old and the youngest was 2 years old. The history reported close contact between the members within the past 10 days. Their upper respiratory tract viral RNA tests were positive for SARS-CoV-2 RNA.
SARS-CoV-2 RNAdetection method: Duplex Real-Time PCR Diagnostic Kit for Rapid Detection of 2019-nCoV ORF1ab/ Ngene.HIV antibodies detection method: the Abbott chemiluminescence method, ZhongxiaoKeju colloidal gold method, Meieril colloidal selenium method, etc. Serum Ab-IgM, Ab-IgGdetection method:colloidal gold method.
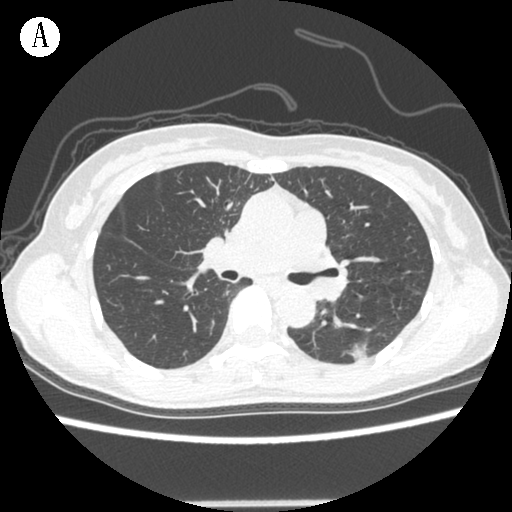
Examination of the positive SARS-CoV-2 and HIV case on the day of admission: T 37.2 ℃, P 86 times / min, R 20 times / min, BP 118 / 81mmHg. Conscious, no skin rashes or subcutaneous bleeding points on the whole body, superficial lymph nodes in the whole body did not display swelling upon clinical touch examination, the breath sounds of both lungs were thick, and no moist rales or rhonchi were heard in the lungs. An abdominal examination revealed no abnormalities. Blood routine test: White blood cells 4.02 10×9/L, lymphocyte count 1.03 10×9/L, CRP0.3 mg/L. Calcitonin < 0.05 ng/mL, and erythrocyte sedimentation rate 14 mm/h. The arterial blood gas analysis was normal. A chest CT (Image A) showed multiple ground-glass nodular-like shadows (GGO) under the left lower lobe pleura. HIV antibodies tested positive. The WB band gp160 gp120 p66 p55 / 51gp41p31p24p17 indicated that the HIV-1 antibody was positive and HIV-RNA 27544cp/ml.HIV-1 resistance measurement shows sensitivity to tenofovir (TDF), lamivudine (3TC), lopinavir / ritonavir (LPV/r), and 16 other drugs. IL-6, IL-10 and TNF-α were not tested. The patient had been separated from her husband for an approximate 2 years and confirmed HIV transmission from her male partner.
The six family members were tested for HIV antibodies, her husband received testing twice, and all presented negative results. All patients provided written informed consent before enrolment in this study. All cases receive ECG examination before receiving drug treatment, particular attention was given to the ECG monitoring of the patient receiving Hydroxychloroquine Sulfate.
On January 22, 2020, the patient's daughter came into proximity with her, arriving from a residence in Hubei, China, after a family gathering. A cluster of infections was reported in Hubei, while other family members had no history of stay in other places.
According to the Treatment Program issued by the National Health and Health Commission of China, the cases in this cluster clearly has only one inducing case; no other potential sources of infection are plausible. This conclusion is based on the history of the first case imported from the Wuhan epidemic area in Hubei, China, one day before the onset of illness. Along with a close contact history, it is clear that six family members had fever, imaging evidence of pneumonia, low or normal white blood cell count or low lymphocyte count, and SARS-CoV-2 RNA positive detection by upper respiratory tract samples. In light of the above diagnostic criteria, the case was diagnosed as COVID-19 common type and an asymptomatic period of HIV infection; her husband was diagnosed with COVID-19 common type, type 2 diabetes; the other 5 cases were diagnosed as COVID-19 common type (Fig. 1).
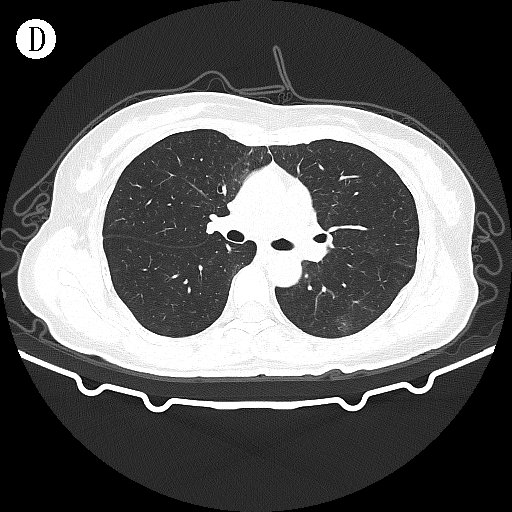
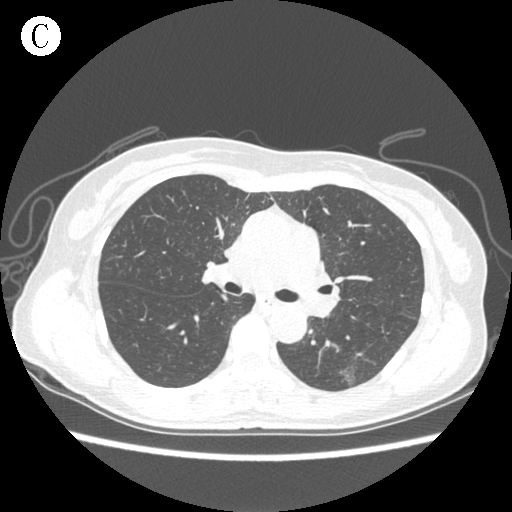
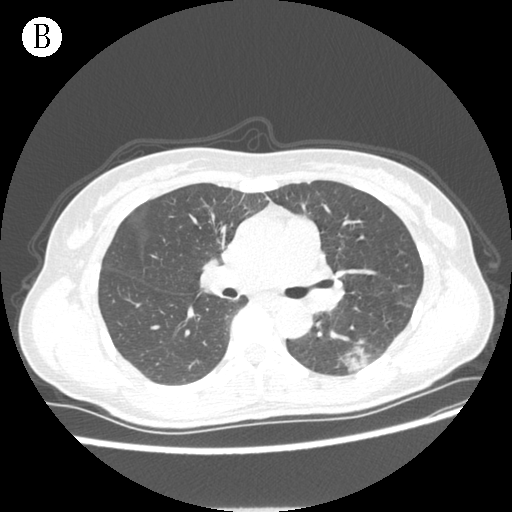
In accordance with the Treatment Program of China, compassionate drug use was given to seven family members 3based on in vitro evidence of SARS-CoV-2 inhibition. Table 1 lists the detailed treatment of this case. Table 2 lists the results of the SARS-CoV-2 RNA test, which continued to be positive, and serum Ab-IgM, Ab-IgG test which continued to be negative. Table 3 lists the comparison reports of CD4 + , CD8 + , and lymphocytes during the treatment. The chest CT lesions increased slightly 5 days after admission (Image B), a small amount was gradually absorbed 14 days after admission, and the chest CT lesions still existed 35 days after admission (Image C). A combined highly effective antiretroviral therapy (HAART) on the 37th day after onset, the following drugs was administered: TDF 300mg once / day, 3TC 300mg once / day, and LPV/r 200 / 50mg twice / Day, etc. On the 50th and 51st days after onset, SARS-CoV-2 RNA test was negative, twice in succession, and chest CT lesions were completely absorbed at 51 days after admission (Image D).
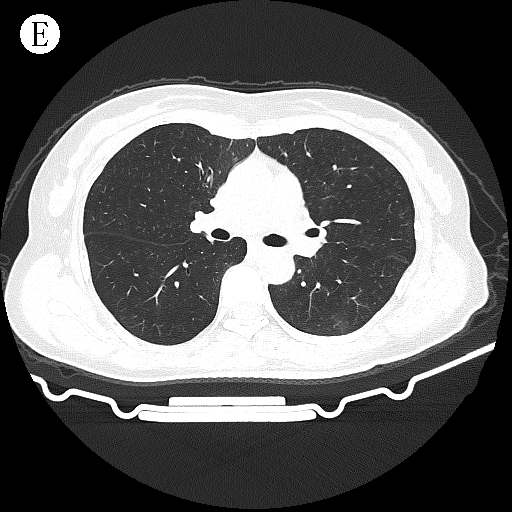
In this case, a follow-up review was conducted on the 2nd and 4th weeks after discharge. Chest CT (Image E) showed no abnormalities, and SARS-CoV-2 RNA, Ab-IgM, and Ab-IgG testing were negative, and COVID-19 has been cured.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}