Our research provides novel insights into the potential utility of dNLR as a diagnostic biomarker for AA in children. To the best of our knowledge, this is one of the few studies to evaluate the accuracy of dNLR as a diagnostic biomarker. We found that using dNLR as a biomarker is an inexpensive and noninvasive approach with good sensitivity and specificity for diagnosing AA in pediatric patients. Our results suggest that incorporating dNLR into daily clinical practice may help expedite diagnosis and reduce the need for additional imaging or further investigation in some cases. These findings are consistent with those of previous studies that have assessed the role of dNLR in other inflammatory and tumoral diseases [9,10].
Early diagnosis is crucial in AA because of the increased risk of appendiceal perforation over time [2]. However, the initial assessment may be challenging, particularly in pediatric patients, as up to 50% of pediatric appendicitis cases present with non-specific symptoms [11]. Moreover, young children may struggle to express their pain, making accurate history-taking and physical examination more challenging in them than in adults [11,12]. Furthermore, the differential diagnosis of AA varies depending on the patient's age. Consequently, several diagnostic tools have been developed to aid in the clinical diagnosis of AA. Among these, abdominopelvic computed tomography is the preferred imaging modality for diagnosis in many centers; however, its use is limited by the risks associated with radiation exposure in children [13]. Magnetic resonance imaging can be employed as an alternative, although some pediatric patients require sedation to undergo these radiologic studies, and the reported failure rate for sedation is as high as 20% [14]. Consequently, the use of ultrasonography (US) in children is increasing [15]. Nevertheless, the accuracy of US findings is operator-dependent, and pediatric sonographers may not be available 24 hours a day. Despite the varied sensitivities and high specificities of US, positive findings can aid clinicians in diagnosing acute appendicitis; however, negative ultrasound findings cannot definitively rule out appendicitis (sensitivity ≈71–94%; specificity ≈81–98%) [16].
In addition, inflammatory parameter tests have been investigated as diagnostic tools. Neutrophils play a significant role in inflammation, macrophage recruitment, angiogenesis, and immune system activation; thus, elevated neutrophil counts are indicative of acute inflammation [17,18]. Based on this premise, several authors have advocated the use of the derived NLR as a diagnostic or prognostic tool for inflammatory, infectious, and tumor diseases in adults [19-21]. Although immunological mechanisms in children differ from those in adults, we hypothesized that a similar concept could be applied to AA in children.
Although dNLR has not been studied in the diagnosis of pediatric appendicitis, a related biomarker, NLR, has been extensively investigated in this context. In a systematic review and meta-analysis encompassing 19 studies and a total of 5,974 pediatric cases, NLR demonstrated an overall sensitivity and specificity of 82% and 76%, respectively, for diagnosing AA [22]. The overall diagnostic odds ratio was 14.34 (95% CI: 9.05–22.73), and the area under the receiver operating characteristic curve was 0.86. These results differ from our findings, which could potentially be attributed to the use of lower cutoff points in some of the included studies. However, Hajibandeh et al. reported a high diagnostic performance of NLR primarily in adult patients [23]. Hence, it can be inferred that the applicability of NLR for diagnosing AA may be more significant in adult populations than in pediatric populations, possibly because of the considerable variation in certain cell types, particularly lymphocytes, at younger ages. Furthermore, optimal NLR cutoff values to detect appendicitis in children vary, ranging from 2.5 to 6.14 [22]. This variation in cutoff values could be explained by variations in patient and control characteristics, clinical settings, laboratory assays, and reference standards.
Moreover, NLR has been employed to differentiate between AA and right ureteral stones, as well as predict the likelihood of uncomplicated versus complicated appendicitis and the development of post-appendectomy abscesses [24-26]. In terms of leukocytes, the aforementioned meta-analysis reported pooled sensitivity and specificity values of 79% and 66%, respectively, for WBC count [22]. We observed comparable diagnostic performance for this parameter, with a higher sensitivity but lower specificity (85% and 56%, respectively). This discrepancy could be attributed to the higher prevalence of complicated appendicitis in our study population, which would have consequently led to an anticipated increase in leukocytosis.
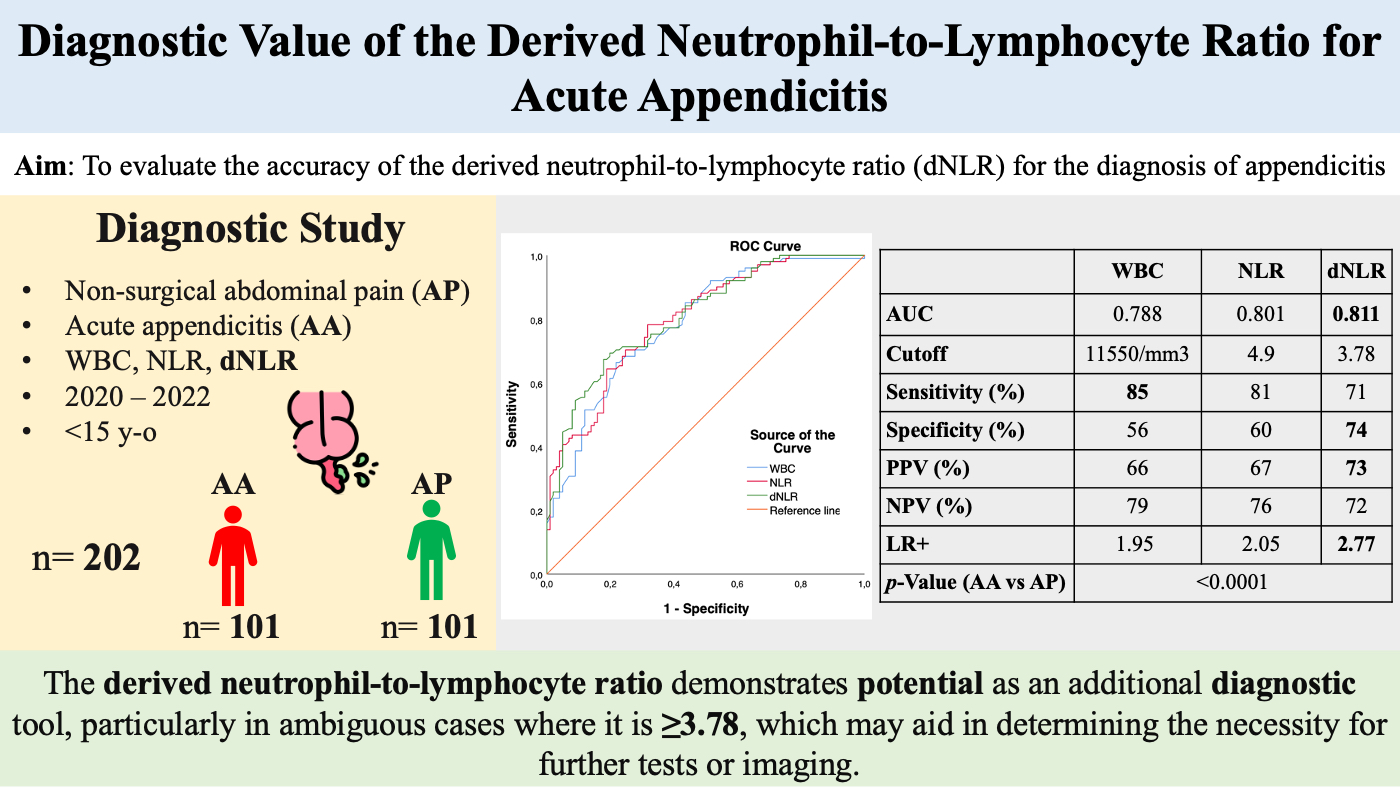
Previous studies have demonstrated that an elevated dNLR in peripheral blood serves as an independent predictor of adverse outcomes in various malignancies, including colon cancer, Hodgkin’s lymphoma, laryngeal squamous cell carcinoma, and prostate and genitourinary tract cancers in adults [27-29]. Another study by Liu et al. found that increased dNLR is an independent and novel predictor of mortality in patients with coronary heart disease who underwent percutaneous coronary intervention (dNLR ≥ 1.96) [30]. In the context of other surgical scenarios, dNLR has also been investigated as a prognostic biomarker in breast cancer patients, aiding in the identification of individuals who would benefit from surgery [31]. Furthermore, in a large cohort of patients with soft tissue sarcoma, multivariate analysis revealed a significant association between elevated dNLR and poor overall survival (hazard ratio: 1.60, 95% CI: 1.07–2.40, p=0.022) [32]. In clinical studies comparing NLR and dNLR, both markers exhibited reliable and sensitive predictive capabilities for in-hospital outcomes in patients with COVID-19 [33]. Unfortunately, the limited number of existing studies on the role of dNLR in diagnosing appendicitis in children makes it challenging to compare our results in a multicenter scenario. A previous study comparing dNLR and other cellular indices in patients with appendicitis and non-surgical AP reported that dNLR is the most accurate parameter, with a cutoff point of 3.98, sensitivity of 70%, and positive predictive value of 77%, consistent with our results, although our cutoff point was higher, which could be explained by the differences in age, sex, types of appendicitis and methodological issues [34]. Moreover, our findings are consistent with existing literature on other inflammatory and infectious diseases. Furthermore, when compared to NLR and WBC count, dNLR appears to be a promising indicator, demonstrating the highest positive predictive value and a positive post-test probability of 73%. This implies that when a dNLR value is ≥3.78, the probability of AA increases from 50% to 73%. Therefore, approximately 1 in 1.3 individuals with a positive test result were diagnosed with appendicitis (Fig. 3). These results suggest that dNLR could serve as a valuable diagnostic tool in guiding the decision to perform additional tests or imaging in cases where dNLR is ≥3.78.
Lymphocyte count can increase in various situations, such as viral infections, which may precede appendicitis or occur concurrently [35]. Furthermore, lymphocyte counts vary considerably in the pediatric population. These factors can significantly impact the interpretation and clinical applicability of NLR. However, considering only neutrophils and leukocytes in the dNLR formula allowed us to elucidate the potential mechanism underlying the elevated dNLR in the systemic inflammatory response of AA. By excluding lymphocytes, dNLR may demonstrate less variability with age, thus ensuring a greater diagnostic applicability for AA across different age groups. Moreover, in the age of AI medicine, affordable and easily accessible laboratory results will become important factors in diagnostic paradigms.
This study had certain limitations. First, it was a single-center study, thus necessitating future research with a multicenter cohort design. Second, further analysis of more substantial datasets is required to establish reference values for dNLR in each age group. This endeavor will enable more objective comparisons in future studies.
{kind=link}