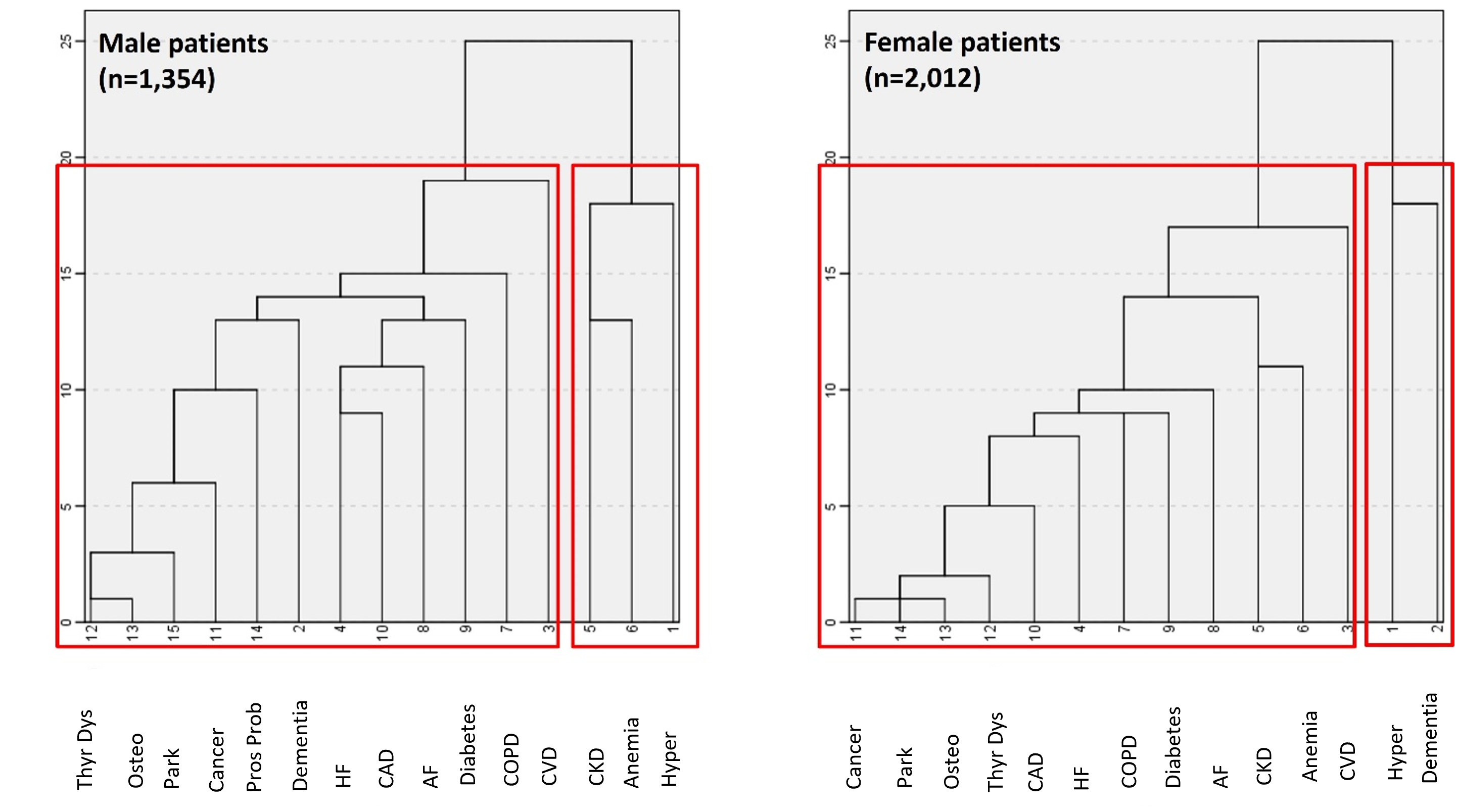
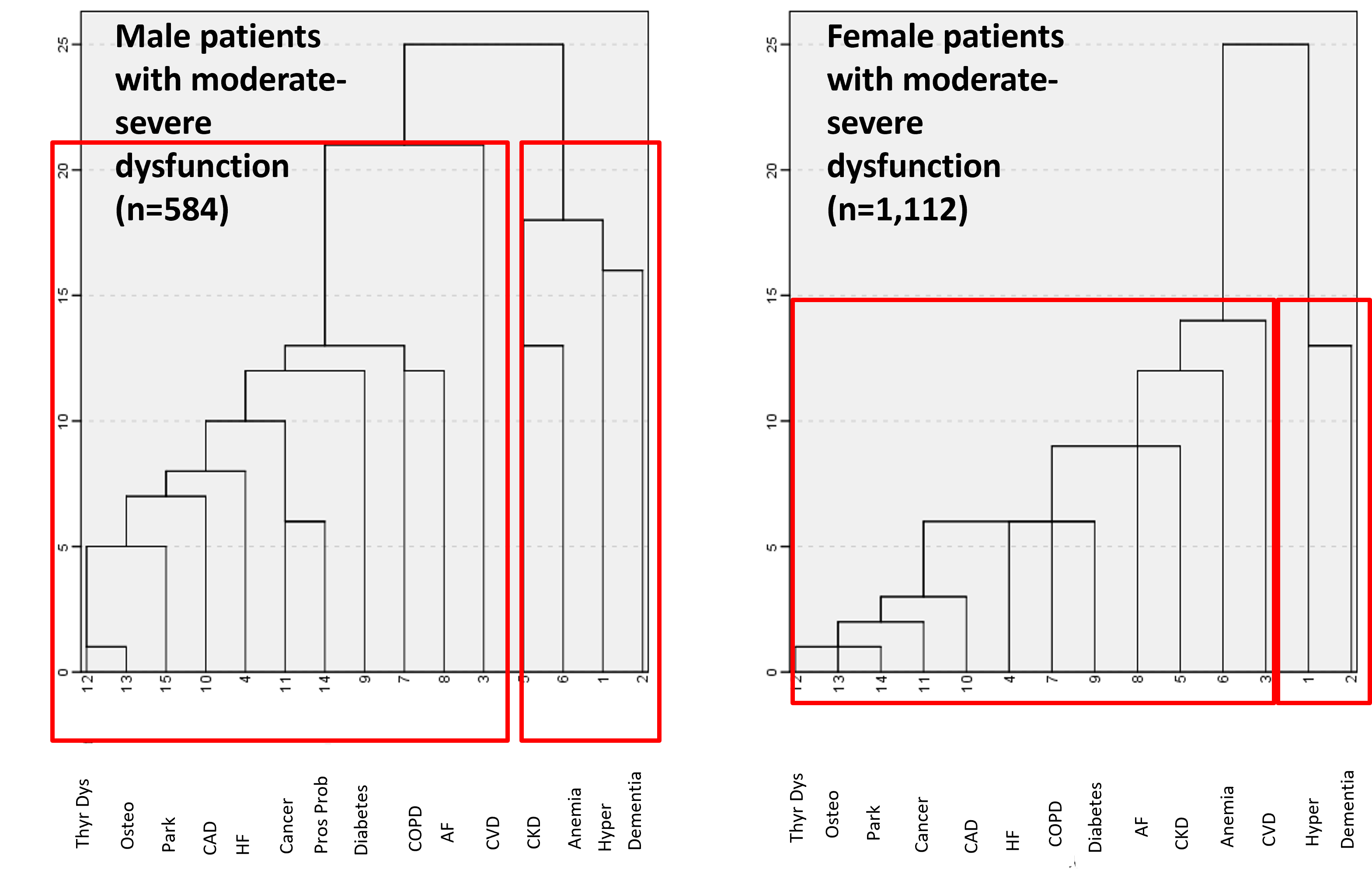
Findings from the present study suggest multimorbidity significantly burdens older individuals discharged from acute care hospitals. Indeed, as already reported in previous studies (33, 35, 41, 42), the occurrence of a single disease without any co-occurring condition was rarely observed in older population. Specifically, in the present study, only 16% of the study cohort was affected by ≤ 1 chronic disease at the time of admission to hospital. Therefore, the great majority of included patients were multimorbid (i.e. with ≥ 2 chronic diseases). In our cohort, most patients had also functional disability: indeed, about 50% of them were moderately-severely dependent, having need of assistance in at least two activities of daily living, and 72.6% were impaired in at least one ADL. However, there was no evidence of a linear strong correlation between number of chronic diseases and degree of functional impairment. Simple count of diseases in fact may be often inadequate to capture the relationship between multimorbidity burden and functional disability; conversely, detailed assessment of disease pairs, MM clusters analysis and assessment of association rules among diseases within the whole cohort and within each MM cluster could improve diagnostic and prognostic stratification of elderly patients. To this regard, our study suggests that MM patterns may change as a function of ADL dependency when explored by cluster analysis or ARM. A sensitivity analysis after stratification by sex found a slight change of composition of MM patterns in both female and male subgroups in comparison with the whole cohort due to a higher prevalence of dementia among women compared to men and a lower prevalence of CKD in very disabled women than in men with similar functional status.
In the whole population, MM cluster analysis displayed a cluster including CKD, anemia, dementia, and hypertension, and a second one including all other chronic diseases. Interestingly, in stratified analysis such clustering could be retrieved only among patients with severe disability, but not among independent patients or those with intermediate degree of dependency. The fact that the cluster CKD-anemia-dementia-hypertension is evident only among patients with the highest functional impairment (ADL = 2) is explainable based on the very high impact of dementia on disability, since dementia causes by definition a variable degree of loss of autonomy in activities of daily living(43, 44). However, all the diseases included in this cluster are known to share common pathophysiological pathways and to interplay in worsening functional status. Specifically, hypertension is one of the most important risk factors for CKD and CKD may cause and/or worsen hypertension, inducing a very dangerous vicious circle (45). Furthermore, CKD and hypertension together may modify gut microbiota, thus potentially impairing the gut-brain axis, which is reported to be relevantly involved in the pathophysiology of cognitive impairment (46). Moreover, epidemiological data supported a higher prevalence of dementia in patients with CKD compared to the general population (47). Finally, CKD is a relevant cause of anemia (48) and their coexistence increases the risk for ADL dependency(49); furthermore, both low hemoglobin and deteriorated kidney function are emerging as risk factors for cognitive impairment and dementia(50–52), and thus potentially ADL impairment. Therefore, the presence of a cluster including CKD, hypertension, anemia and dementia in our cohort and in patients with at least 2 disabilities is not surprising at all and these findings resulted to be very plausible from both a biological and epidemiological point of view.
With respect to ARM analysis, in the whole cohort, the strongest lift linked the association of CAD and AF as antecedent condition with HF as subsequent condition. This association was found to be strong also in various subgroups of patients with different functional status, suggesting that is relevant regardless of the degree of disability. Of note, the causal relationship among CAD, AF and HF is largely supported by the literature(53) and contributed to the highest lifts of ARM patterns including HF and AF in previous studies(32). Stratification by functional status and cluster analysis significantly changed the strength and distribution of ARM patterns; in particular, the highest lifts characterised the combinations of AF-anemia and CKD in functionally independent patients and mildly dependent ones; most significant ARM patterns in highly dependent patients were represented by CAD-HF and AF in cluster 1, hypertension-anemia and CKD followed by dementia-CKD-anemia and hypertension in cluster 2. These findings confirm that aggregation of distinct disease conditions significantly change in function of ADL performance and many chronic diseases may interact each other to impact functional status; the association between AF-anemia and CKD in functionally independent patients is confirmed by previous 2-sample mendelian randomization study, showing a bidirectional causal relationship between anemia and cardiovascular diseases including AF (54); furthermore, CKD and AF seem to be pathophysiologically interrelated, sharing several molecular mechanisms, including inflammation, aberrant activation of renin-angiotensin-aldosterone system and dysregulation of calcium homeostasis(55). Previous studies have shown that AF, CKD, and HF were variably associated with functional impairment(15, 56, 57); the coexistence of the three diseases in functionally independent patients may capture a segment of the geriatric population with mild disease severity and preserved functional performance; such patients still deserve accurate follow-up evaluations to promptly detect changes in the functional performance potentially due to chronic disease progression.
Interestingly, in the transition from no to mild functional impairment, COPD emerged as a diagnosis in most significant ARM patterns with COPD-AF-anemia and CKD being the most significant rule. Of note, COPD was reported to be independently associated to AF, probably due the combined effects of pulmonary hypertension, hypoxemia, hypercapnia, oxidative stress and inflammation, on the risk of atrial arrythmia(58). Additionally, some reports have suggested a potential link between COPD and anemia(59), as well as between COPD and CKD(60), but further studies will be needed to clarify the real clinical impact of the coexistence of these comorbidities on functional status. However, a previous study on community-dwelling patients has shown that patients with COPD experience only mild ADL disability and more severe IADL dependency(61), thus confirming results of our study. Furthermore, COPD may affect skeletal muscle metabolism and bioenergetics(62), thus potentially contributing to the onset of physical disability.
Finally, ARM patterns in most disabled group underlined the potential impact of cardiovascular diseases, and CVD in cluster 1, as well as depicting underlying relationships between CKD, anemia, and dementia in cluster 2; although CVD is recognized as a known risk factor for severe functional and cognitive impairment in the older population, the functional impact of cardiovascular diseases is highly variable depending on disease severity, type and population setting(57). Indeed, among highly disabled patients, less impactful diseases like AF and hypertension were consistently replaced by CAD and HF in most significant rules; the impact of CAD and CVD on physical disability was recently confirmed by Kodera et al. in community-dwelling Japanese adults(63), among whom history of CVD and CAD substantially led to similar functional dependency; among patients belonging to cluster 2, the most significant rules involved the triad CKD-hypertension and anemia with or without dementia; this finding confirms that multimorbidity patterns of CKD change depending on functional status as already reported in community-dwelling older patients (15); interestingly, aggregation of CKD with hypertension and anemia may intercept patients with moderate-severe CKD stage, who are at increased risk of severe ADL impairment and sarcopenia(64–67). However, lack of information about disease severity did not allow us to confirm this hypothesis. As such, future studies including both prevalence and severity of chronic diseases are needed to disentangle the complex relationship between MM patterns and ADL disability.
Our study has several limitations: first, lack of information about the clinical severity of chronic diseases affecting older patients may have affected the change in MM patterns across ADL groups; second, the group of moderately-severely disabled patients included patients with a high range (from 2 to 8) of disabled ADL; this heterogeneity might have affected the reproducibility of the study findings; third, MM patterns’ overlapping between whole cohort and moderately-severely dependent patients may be due to the relative high prevalence of high ADL impairment in our study population with potential loss of information in less represented groups.
Faced to these limitations, our study has also some strengths. First, this is a real-word study potentially able to give useful insights about the clinical presentation in routine medical practice of older patients with different degrees of disability. Second, the sample size of the included cohort is relatively large (n = 3336). Third, sex-stratified sensitivity analyses conducted to test the robustness of study findings substantially confirmed our results, with only slight differences in disease distributions, mainly due to different prevalence of high-impact diseases, such as CKD and dementia.
In conclusion, our study suggests the existence of a link between different pattern of MM and functional impairment. Further prospective multicentric studies including prevalence and severity of chronic diseases will be needed to confirm these findings.
{kind=link}
{kind=link}