Background characteristics of the patients.
Table 1 summarizes clinical characteristics of the patients. Male patient ratios of ECPELLA (76%) and IABP + VA-ECMO (74%) groups were higher than VA-ECMO group (50%, p = 0.02). Bystander-CPR rate in VA-ECMO was higher than other groups (83% in ECPELLA, 85% in IABP + VA-ECMO, and 98% in VA-ECMO, respectively, p = 0.03). While shockable rhythms were seen in both ECPELLA (48%) and IABP + VA-ECMO (47%) groups, no cases were seen in VA-ECMO group (0%, p < 0.001). Pulseless electric activity in VA-ECMO was higher than other groups (41% in ECPELLA, 47% in IABP + VA-ECMO, and 88% in VA-ECMO, respectively p < 0.001). Rates of out of hospital cardiac arrest (OHCA) were higher in ECPELLA (41%) and IABP + VA-ECMO (42%) compared to VA-ECMO (19%, p = 0.02). Higher rates of acute coronary syndrome were seen in ECPELLA (66%) and IABP + VA-ECMO (56%) compared to VA-ECMO (24%, p = 0.0003). Both Door to ECMO time (23 min in ECPELLA, 36 min in IABP + VA-ECMO, and 39 min in VA-ECMO, p = 0.005) and Collapse to ECMO time (27 min in ECPELLA, 49 min in IABP + VA-ECMO, 36 min in VA-ECMO, p = 0.004) were shorter in ECPELLA group.
Changes in hemodynamic parameters, serum lactate, and Vasoactive Inotrope Score.
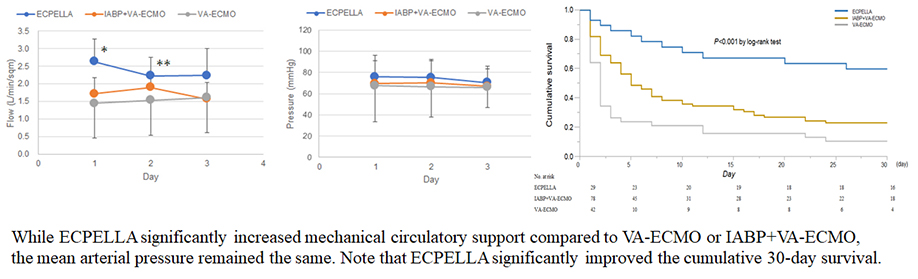
Figure 2A shows changes in MCS flows from support day 1 to day 3. The ECPELLA group was significantly higher MCS flow than other groups on days 1 and 2 (P < 0.05). While mean arterial pressure (Fig. 2B) was similar among treatment groups, VA-ECMO group showed significantly higher mean main pulmonary artery pressure (mPAP, Fig. 2C) and the central venous pressure (CVP) on day 1 compared to other groups (P < 0.05, Fig. 2D).
While rates of serum lactate levels more than 4mmol/L (Lact-4) were decreased from E-CPR to support day 3 in all groups, VA-ECMO group was higher than other groups at E-CPR. On support day 1, IABP + VA-ECMO group showed the highest rates of Lact-4 among groups. On days 2 and 3, the rates of Lact-4 in VA-ECMO group were higher than other groups and ECPELLA group showed the lowest Lact-4 rates among groups (Fig. 3 left panel).
The Vasoactive Inotrope Score was calculated as dopamine dose (µg/kg/min) + dobutamine dose (µg/kg/min) + 100 × epinephrine dose (µg/kg/min) + 10 × milrinone dose (µg/kg/min) + 10000 × vasopressin dose (unit/kg/min) + 100 × norepinephrine dose (µg/kg/min). While the rate of VIS more than 10 (VIS-10) of IABP + VA-ECMO group was lower than other groups on day 1, both IABP + VA-ECMO and ECPELLA showed lower VIS-10 rates on days 2 and 3 compared to VA-ECMO group suggesting VA-ECMO group required more vasoactive inotropes from MSC support days 1 to 3 (P < 0.05, Fig. 3).
VA-ECMO weaning and rate of Cerebral Performance Category Score 1 or 2.
The VA-ECMO weaning rates were 62% in ECPELLA, 44% in IABP + VA-ECMO, and 17% in VA-ECMO, respectively. The VA-ECMO weaning rate in ECPELLA group was significantly higher than other groups (P = 0.0002). Rates of Cerebral Performance Category 1 or 2 in ECPELLA, IABP + VA-ECMO, and VA-ECMO groups were respectively 31%, 13%, and 7% indicating that ECPELLA group had better neurological outcome compared to other groups (P = 0.02) (Table 2).
Cumulative 30-day survival rates and factors affecting survival.
The Kaplan-Meier survival analysis revealed that cumulative 30-day survival rates were 55% in ECPELLA, 23% in IABP + VA-ECMO, and 9.5% in VA-ECMO, respectively (P < 0.001, Fig. 4). Multivariate Cox regression analysis for 30-day survival revealed that older age (per 10 years-old increment, HR: 1.30, 95% confidential interval (95%CI): 1.13–1.52, p = 0.005) and longer Collapse to VA-ECMO Time (per 10-minute increment, HR: 1.22, 95%CI: 1.13–1.31, p < 0.0001) increased the risk of survival. Among treatment modalities, ECPELLA significantly reduced the risk of 30-day survival compared to IABP + VA-ECMO (HR: 0.46, 95%CI: 0.24–0.88, P = 0.02, Table 3), whereas single VA-ECMO significantly increased the risk compared to IABP + VA-ECMO treatment (HR: 1.86, 95%CI: 1.16–2.99, P = 0.01, Table 3).



{kind=link}