To the best of our knowledge, this is the first study to develop and validate a convenient and practical dynamic nomogram for detecting AKI in ICU patients with cirrhosis using the MIMIC IV 2.0 database. AKI risk prediction models facilitate medical decision-making when critically ill patients with cirrhosis are admitted to the ICU and facilitate early identification or implementation of preventive measures to improve the prognosis of AKI. Multiple studies have reported prediction models for AKI in different clinical settings [8, 16, 21, 22]. However, the number of cases in these studies was small, and a prediction model for AKI in critically ill patients with cirrhosis is lacking. The increase in the computerization of ICU has generated large electronic databases that are suitable for "big data" research. Using machine learning algorithms to analyze large datasets and develop models for prognostication or decision support in critical care could be a cost-effective alternative to biomarkers for AKI prognostication.
In recent years, a specific modern technique, the least absolute shrinkage and selection operator (LASSO), has attracted much attention [23]. Traditional regression techniques are limited in the analysis and synthesis of large numbers of covariates, including multicollinear variables, but thus far, the majority of the data on AKI and cirrhosis have utilized traditional statistical techniques [21]. LASSO is a regression-based methodology that allows for a large number of covariates in a model. Importantly, it has the unique characteristic of penalizing the absolute value of a regression coefficient; thus, regulating the influence a coefficient may have on the overall regression. The greater the penalization, the greater the coefficient shrinkage, with some coefficients reaching zero, thus automatically removing unnecessary/uninfluential covariates [24]. The logistic LASSO model can actively select from a large and potentially multicollinear set of variables in the regression, resulting in a more relevant and interpretable set of predictors [25]. Therefore, in the present study, we aimed to investigate the relationship between baseline characteristics, vital signs, laboratory test results, and other risk factors on acute kidney injury in critically ill patients with cirrhosis.
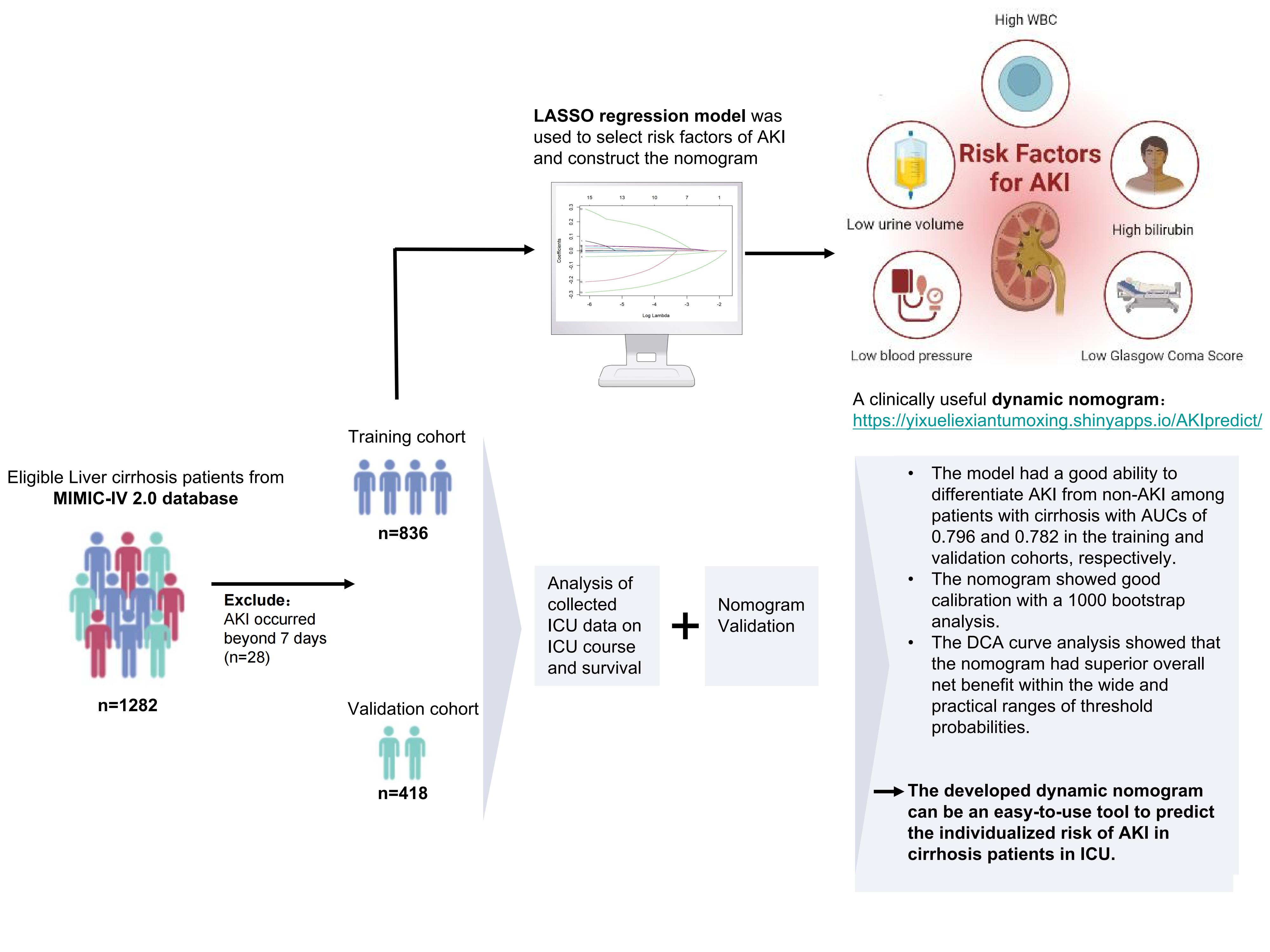
Our study has several strengths. Most of the major risk variables associated with AKI were included in the study, and the risk model development was based on parameters available to clinicians, thereby providing clinically relevant information in the management of patients with cirrhosis. MAP, UV, WBC, TB, and GCS were included in this nomogram, making it an objective and simple-to-use tool to screen patients for AKI in a dynamic online manner. The proposed dynamic nomogram showed good performance in discrimination, calibration, and clinical application, providing valuable information for the decision-making of appropriate therapy options for individual patients. Moreover, it fills the gap between the high incidence of AKI in cirrhosis and the lack of a reliable clinical predictive model. Our findings also confirm that the mortality of AKI patients in the ICU is high, and the length of hospital stay (LOS) is increasing, which supports the necessity of identifying high-risk patients. These patients could benefit from monitoring and primary prevention strategies to reduce the incidence of AKI.
Our model showed that lower mean arterial pressure, urine volume, GCS, higher white blood cell count, and total bilirubin were related to the occurrence of AKI in patients with cirrhosis. The risk factors we used for the identification of AKI were consistent with previous AKI literature. The kidneys account for less than 5% of our body weight but receive approximately 25% of our cardiac output. Therefore, targeting adequate renal perfusion is considered a potential factor in changing the risk of AKI [26]. Mean arterial pressure (MAP) is widely used as an index for optimal blood pressure, and previous studies have shown that the incidence of serious renal adverse events is higher in patients with lower blood pressure [27, 28]. A decreased urine output may be the first sign of renal function loss; however, it is frequently not reported in publications for practical reasons [21]. Our study shows the importance of urine volume in predicting the occurrence of AKI; therefore, urine volume should be evaluated in future studies [29]. In the ICU, the GCS scoring system is commonly used to evaluate the severity of a patient’s condition. Our results revealed that patients with a low GCS score were more likely to develop AKI, which is consistent with previous studies [30, 31]. Infection, particularly sepsis, is the most important risk factor for renal function [32]. A high WBC count, a surrogate of systemic inflammation, is a known independent predictor of mortality in patients with advanced cirrhosis and is a driver for the development of AKI [33]. Elevated WBC count has also been found to be associated with renal dysfunction in patients with spontaneous bacterial peritonitis (SBP) [34] and alcoholic hepatitis [35]. Hyperbilirubinemia can be found in 60% of AKI patients. Elevated serum bilirubin levels are an independent risk factor for AKI [36]. An increase in bilirubin can induce oxidative stress in renal tubular cells, induce apoptosis, aggravate renal ischemia-reperfusion injury, and lead to AKI [37, 38].
This study has several limitations. First, although it was performed in a large cohort, selection bias might be unavoidable because this study was a retrospective analysis of secondary data. Second, the model was constructed based on a US population and developed and validated using the same database. Thus, its generalizability to the global population remains unclear. It was more reliable to validate it prospectively or at least in another database. Third, considering that the mean AKI occurrence time was within 7 days after admission, we only collected data for a week after the onset of admission. Although this part of the population is relatively small, it still exists; therefore, our model may not be as good at predicting late AKI. Fourth, we only considered traditional parameters and did not consider some valuable biomarkers (e.g., cystatin C and neutrophil gelatinase-related lipoid) that might contribute to AKI development. Therefore, future studies are needed to assess these kidney biomarkers to substantiate their roles as clinical tools and assess whether the addition of biomarkers enhances prediction.
{kind=link}