3.1 Significant differences in MRPL17 expression and assessment of MRPL17 as a pan‑cancer prognostic biomarker
We explored MRPL17 expression in tumor and normal tissues from the TIMER database and found that MRPL17 was significantly upregulated in 19 cancer types, including BLCA, BRCA, CESC, CHOL, COAD, ESCA, GBM, HNSC, KIRC, KIRP, LIHC, LUAD, LUSC, PAAD, PRAD, READ, STAD, THCA and UCEC. However, MRPL17 was downregulated only in KICH (Fig. 1A). The result of comparison of MRPL17 expression of the pan-cancer with normal tissues in the Sangerbox 3.0 web showed that MRPL17 mRNA expression was significantly high among most cancer types except PRAD and KICH, which was consistent with the TIMER database results (Fig. 1B). We further analyze the cancers without normal tissues in the TIMER database via the GEPIA database, and the results showed that MRPL17 was significantly upregulated in DLBC, LAML, TGCT, THYM and UCS. However, MRPL17 was downregulated only in LAML (Fig. 1C). We downloaded data of tumor cell lines from the CCLE database and analyzed the expression of MRPL17 in multiple tumor cells (Fig. 1D). From the result, it was observed that the expression level of MRPL17 was significantly different in cancer cell lines (Kruskal Wallis test p < 0.001) of different tissue origins.
We further explored the IHC results in HPA database to figure out MRPL17 expression in tumors. The result showed that normal breast, colon, kidney, liver, lung and stomach had negative or medium MRPL17 IHC staining, but tumor tissues showed medium or strong IHC staining (Fig. 2).
3.2 Prognostic value of MRPL17 across cancer types
To further elucidate the effect of FAM110A expression on the prognosis of patients with cancer, we downloaded TCGA RNA-seq and clinical data. Univariate COX regression analysis was performed to explore the relationship between MRPL17 expression and overall survival (OS) in 33 cancer types, as shown in Fig. 3A. High expression of MRPL17 was significantly associated with poorer prognosis in patients with ACC, KICH, KIRC, LAML, LGG, LIHC, LUAD and UVM (Fig. 3C-J).
To exclude the bias caused by non-tumor events, we further evaluated the effect of MRPL17 expression levels on disease-specific survival (DSS) (Fig. 3B). The results were roughly consistent with the OS analysis, demonstrating that high MRPL17 expression was associated with poor prognosis in patients with ACC, KIRC,KIRP,LGG, LIHC, LUAD and UVM (Fig. 3K-Q).
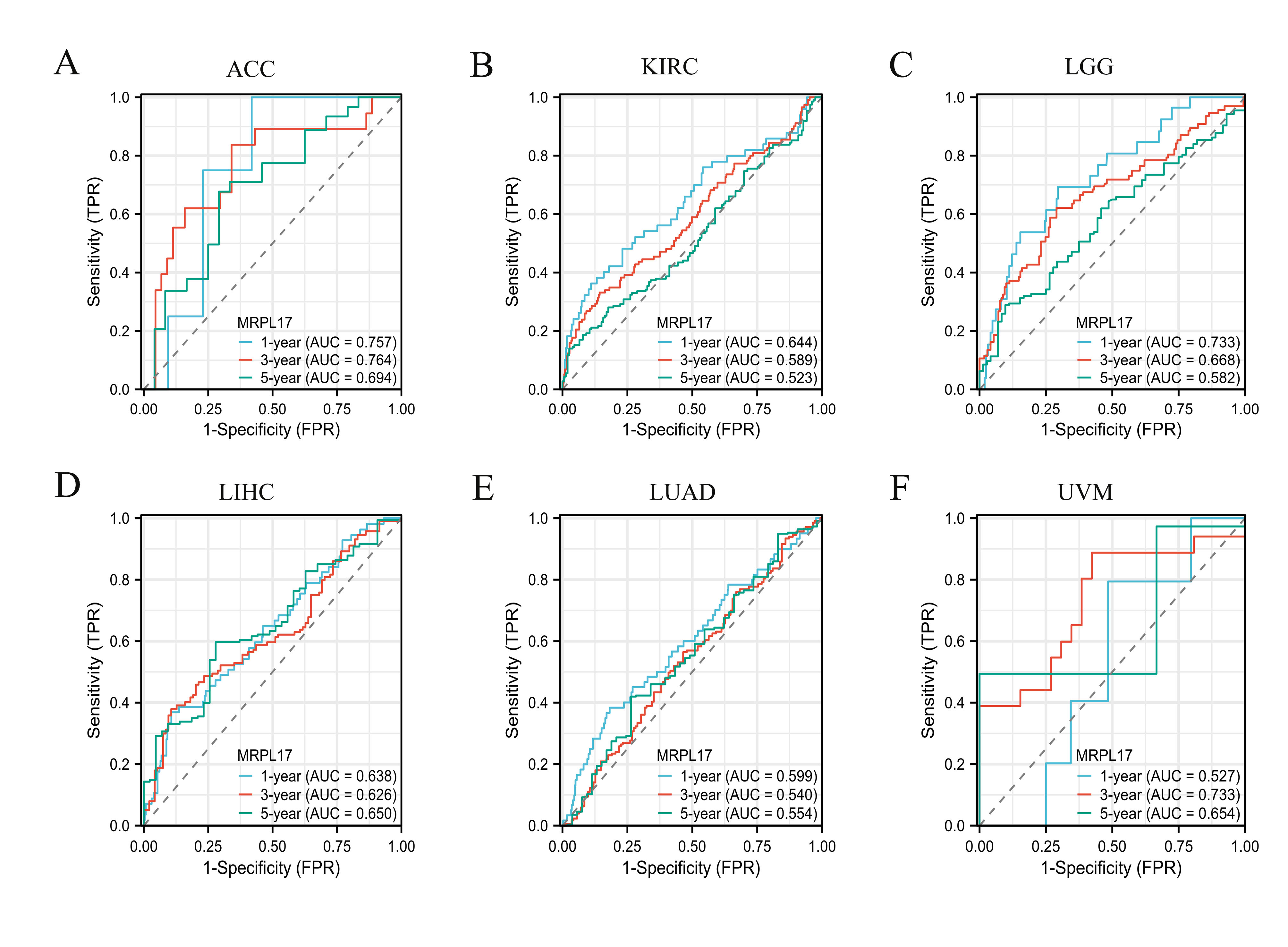
Therefore, MRPL17 overexpression in ACC, KIRC, LGG, LIHC, LUAD and UVM had shorter OS and DSS. Moreover, the time-dependent ROC curve indicated that the 1-, 3-, and 5-year OS of MRPL17 were above 0.5 in ACC, KIRC, LGG, LIHC, LUAD and UVM (Figure S1). These results revealed that MRPL17 expression levels are significantly associated with prognosis in patients with multiple tumor types.
3.3 Mutation Analysis of MRPL17
We discussed MRPL17 genetic alterations in pan-cancer using the cBioPortal database. Mutation, amplification, deep deletion and are the main type of frequent genetic alterations of MRPL17. The frequency of genetic variation of MRPL17 was the highest in Glioma (3.7%) and was mainly in the form of deep deletion. The second and the third highest frequency of MRPL17 occurred in pheochromocytoma and ACC (Fig. 4A). Moreover, we showed additional genetic alterations and their locations within MRPL17(Fig. 4B).
3.4 Correlation of MRPL17 expression on immune checkpoints and immunotherapy
Since the expression of immune checkpoint genes is closely related to the efficacy of immunotherapy, we first explored the relevance of MRPL17 to genes that are recognized as immune response-related checkpoints using the TCGA database. Interestingly, two significant but diametrically opposite trends were observed among the different cancers (Fig. 5A). Next, we verified the correlations between MRPL17 and several immune checkpoint blocker genes, including PD1, PD-L1, CTLA-4 and LAG-3, in the TIMER 2.0 database. The most significant positive correlation between MRPL17 and these genes was observed in LIHC and UVM, and the most significant negative correlation was observed in LUSC (Fig. 5B-E; Supplementary Table 1).
We also performed the correlation analysis between MRPL17 expression and TMB and MSI, which were significantly linked with immune checkpoint inhibitor (ICIs) sensitivity. A significant positive correlation was observed between MRPL17 and TMB in ACC, KIRC, LGG, LUAD, PAAD, SARC, SKCM, STAD, UCEC and UCS (Fig. 5F). MRPL17 displayed a positive association with MSI in KIRC, STAD, UCEC and UVM, and a negative association in LGG (Fig. 5G).
3.5 Correlation of MRPL17 expression with immune infiltration
We investigated the link between MRPL17 expression and tumor purity. We utilized the ESTIMATE algorithm to calculate the stroma score, immune score, and estimate score of relevant tumor samples based on the TCGA database and assessed the correlation between MRPL17 expression levels and those scores. Based on our data, the three cancer types that showed the strongest association between MRPL17 and the stroma score were UVM, TGCT and PAAD. The three tumor types that showed the strongest association between MRPL17 expression and immune score were UVM, PAAD and LUSC. The three tumor types that showed the highest association between MRPL17 and estimate scores were UVM, PAAD and LUSC (Fig. 6A). In addition, we also analyzed the relationship between MRPL17 expression and immune cell infiltration using TIMER. The most obvious positive correlation between immune cell infiltration and MRPL17 was found in LIHC. The expression of MRPL17 was positive correlation with dendritic cells (DC) in most tumors, with CHOL being the most significant. MRPL17 expression showed a negative correlation with CD4 T cells in most tumors (Fig. 6B).
To determine whether MRPL17 expression predicts the therapeutic effect of immunosuppressants, we analyzed the correlation between MRPL17 expression and the immunophenoscore (IPS), which was conducted from a panel of immune-related genes belonging to the four classes-effector cells, immunosuppressive cells, MHC, and selected immune checkpoints30. IPS predicted outcomes in melanoma patients treated with the CTLA-4 and PD-1 blockers31. We found that MRPL17 was positively linked to EC and negatively linked to CP in most cancers (Fig. 6C). IPS analysis demonstrated the ability of MRPL17 to predict PD- 1/PD- L1 blockade responses in various cancers.
3.6 Tumor stemness and MRPL17 expression
Cancer progression involves the gradual loss of a differentiated phenotype and the acquisition of progenitor and stem-cell-like features. Tumor stemness is associated with suppressed immune response, higher intratumoral heterogeneity, and dramatically worse outcome for the majority of cancers26. Therefore, we further investigated the relationship between MRPL17 expression and tumor stemness scores on 6 different dimensions using the Sangerbox platform. We found a significant positive correlation between MRPL17 expression and tumor stemness scores calculated by mRNA expression and methylation signature in most malignant tumors, especially STES, STAD, PAAD, SARC and PCPG (Fig. 7 and Supplementary Table 2), suggesting that tumors with high MRPL17 expression often contribute to stemness maintenance.
3.7 Single-Cell Functional Analysis of MRPL17
To further study the latent role of MRPL17 in tumors, we investigated the function of MRPL17 at the single-cell level using CancerSEA (Fig. 8A). The findings displayed that MRPL17 was positively linked with DNA damage, DNA repair and stemness of acute lymphoblastic leukemia (ALL). In BRCA, MRPL17 had a positive relationship with DNA repair and inflammation and had a negative relationship with metastasis. In LUAD, MRPL17 had a positive relationship with proliferation and DNA damage and had a negative relationship with quiescence. In OV, MRPL17 had a positive relationship with apoptosis and had a negative relationship with invasion, proliferation and DNA repair. In PRAD, MRPL17 had a positive relationship with DNA repair and had a negative relationship with EMT and proliferation. However, MRPL17 had a negative relationship with quiescence, DNA damage, apoptosis, DNA repair and metastasis in UVM (Fig. 8B).
3.8 Drug Sensitivity Analysis
We used Gene Set Cancer Analysis (GSCA) to investigate the drug sensitivity of MRPL17 expression in tumors. MRPL17 expression was negatively associated with 50% inhibitory concentration (IC50) values of TGX221 and dabrafenib. Moreover, there was a positive correlation between MRPL17 expression and IC50 values of 20 types of drugs, such as AT-7519, AZD8055, BHG712, BIX02189, BMS345541, CP466722, I-BET-762, KIN001-102, Masitinib, NPK76-II-72-1, OSI-027, PIK-93, TG101348, TL-1-85, TL-2-105, TPCA-1, Vorinostat, WZ3105, YM201636 and ZSTK474(Fig. 9).
3.9 Protein Interaction Network and Enrichment Analysis of MRPL17
To further explore the role of XRCC4 in tumorigenesis, we screened out the targeting MRPL17-binding proteins and the XRCC4 expression-related genes for enrichment analyses. Via the STRING database, we obtained 50 MRPL17-binding proteins, which showed the protein–protein interactions network (Fig. 10A). Next, we obtained the top 100 MRPL17 expression-related genes via the GEPIA2 database. Biological process (BP) enrichment analysis showed that MRPL17-related genes were mainly involved in ribonucleoprotein complex biogenesis, ribosome biogenesis and RNA localization. Molecular function (MF) enrichment analysis showed that the role of MRPL17 in tumor pathogenesis was related to structural constituent of ribosome, threonine-type peptidase activity and threonine-type endopeptidase activity. We found that MRPL17-related genes were enriched in the peptidase complex, endopeptidase complex and proteasome complex in cellular component (CC) enrichment analysis. In addition, KEGG pathway analysis showed that MRPL17 participated in some pathways, such as amyotrophic lateral sclerosis, huntington disease and proteasome (Fig. 10B).
3.10 MRPL17 Is Regarded as an Independent Marker in LIHC
We used logistic regression analysis to estimate the correlation between MRPL17 expression and clinical characteristics in LIHC and PAAD from TCGA database. Univariate analysis confirmed that pathologic T stage, pathological M stage, pathologic stage, MRPL17 expression and tumor status were important prognostic factors of OS in LIHC. MRPL17 expression and tumor status were identified as independent prognostic factors in LIHC by multivariate analysis (Table 2).
Moreover, the IHC analysis also exhibited high expression of MRPL17 in tumors relative to normal tissues (Fig. 11A). Three indicators—IHC mean density, IHC H-Score and IHC IRS —all supported MRPL17 expression dramatically increased in 39 paired tumor tissues (Fig. 11B). These results indicated that AARS2 may perform oncogenic functions in LIHC.
Table 2
Univariate and Multivariate Cox analysis of OS in TCGA-LIHC dataset.
| Characteristics | Total(N) | Univariate analysis | | Multivariate analysis |
| Hazard ratio (95% CI) | P value | Hazard ratio (95% CI) | P value |
| Pathologic T stage | | | | | | |
| T1&T2 | 277 | | | | | |
| T3&T4 | 93 | 2.598 (1.826–3.697) | < 0.001 | | 2.029 (0.274–15.024) | 0.489 |
| Pathologic N stage | | | | | | |
| N0 | 254 | | | | | |
| N1 | 4 | 2.029 (0.497–8.281) | 0.324 | | | |
| Pathologic M stage | | | | | | |
| M0 | 268 | | | | | |
| M1 | 4 | 4.077 (1.281–12.973) | 0.017 | | 1.179 (0.280–4.959) | 0.822 |
| Pathologic stage | | | | | | |
| Stage I&Stage II | 259 | | | | | |
| Stage III&Stage IV | 90 | 2.504 (1.727–3.631) | < 0.001 | | 1.298 (0.177–9.528) | 0.798 |
| MRPL17 | | | | | | |
| Low | 187 | | | | | |
| High | 186 | 1.700 (1.199–2.411) | 0.003 | | 2.177 (1.363–3.478) | 0.001 |
| Histologic grade | | | | | | |
| G1&G2 | 233 | | | | | |
| G3&G4 | 135 | 1.091 (0.761–1.564) | 0.636 | | | |
| Tumor status | | | | | | |
| Tumor free | 202 | | | | | |
| With tumor | 152 | 2.317 (1.590–3.376) | < 0.001 | | 1.916 (1.198–3.064) | 0.007 |
{kind=link}