3.1 Preparation and characterization of the copolymer and nanoparticles
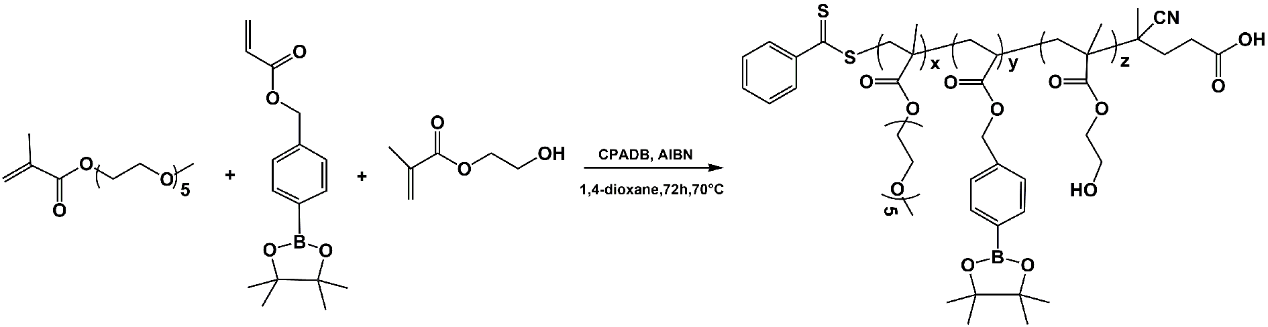
The copolymer PBE30-r-HEMA10-r-PEGMA30 was synthesized via RAFT polymerization, as outlined in Scheme 1. The chemical structure of PBE30-r-HEMA10-r-PEGMA30 was elucidated using 1H NMR spectroscopy (Fig. 1A). Comparative analysis with the 1H NMR spectra of the individual HEMA, PEGMA, and PBE monomers (Figures S1-S3) revealed the absence of double bond proton peaks, retention of characteristic peaks from the three monomers, and emergence of new proton peaks from the main chain at 0.8–2.5 ppm in the copolymer spectrum (Fig. 1A). Consequently, the 1H NMR data validated the successful synthesis of PBE30-r-HEMA10-r-PEGMA30. Functioning as an amphiphilic copolymer, PBE30-r-HEMA10-r-PEGMA30 demonstrated the ability to self-assemble into nanoparticles using a nano-precipitation technique, denoted as NPSPHE. The nanoparticles were composed of a hydrophilic PEGMA/HEMA shell and a hydrophobic PBE core. The PEGMA component improved water solubility and extended circulation time, while HEMA promoted cell adhesion. The PBE core was designed to degrade in the presence of excessive ROS, facilitating effective drug delivery in disease microenvironments.27–31 The size and distribution of the nanoparticles (NPSPHE) were determined using DLS, revealing an average size of 163.2 ± 4.87 nm (Fig. 1B). TEM analysis showed that NPSPHE exhibited spherical structures (Fig. 1C). The CMC of NPSPHE was measured using the Nile red fluorescent method, yielding a value of 0.039 mg/mL (Fig. 1D). To create drug-loaded nanoparticles, the PBE30-r-HEMA10-r-PEGMA30 copolymer was combined with EOFAZ to form self-assembled nanoparticles (NPSPHE@EOFAZ) via the nano-precipitation method. The size of NPSPHE@EOFAZ was 189 ± 0.54 nm (Fig. 1E), with a spherical morphology (Fig. 1F). The observed changes in size and morphology of NPSPHE@EOFAZ compared to NPSPHE were attributed to the incorporation of EOFAZ into the nanoparticles. Due to the hydrophobic nature of EOFAZ, its dialysis out of the aqueous solution during preparation was minimal, leading to the assumption that the final amount of EOFAZ in NPSPHE@EOFAZ was the initially added quantity.32 Consequently, the drug loading and encapsulation efficiency of EOFAZ were not further investigated based on previous laboratory findings.
The stability of NPSPHE and NPSPHE@EOFAZ was assessed in various media, as depicted in Fig. 1G-H. Both NPSPHE and NPSPHE@EOFAZ were stored in PBS at 4°C, maintaining their size for 7 days. In DMEM (with 10% FBS) at 37°C, the particle size remained constant for 48 h. These findings demonstrate the robust stability of NPSPHE and NPSPHE@EOFAZ across different media. Gavage administration, known for its patient-friendly and long-term use benefits, facilitates drug absorption through the gastrointestinal tract into systemic circulation, resulting in reduced drug intake and bioavailability. For effective gastric medication, tolerance to the gastrointestinal tract's acidity and alkalinity is crucial. Therefore, we simulated strong acidic stomach conditions using a hydrochloric acid buffer (pH 1.5), and intestinal conditions with acetic acid buffer (pH 4.6) and phosphate buffer (pH 6.8) to evaluate NPSPHE and NPSPHE@EOFAZ stability. Both formulations remained stable for at least 18, 24, and 48 h in pH 1.5, 4.6, and 6.8 buffer solutions, respectively. Although stability in acidic environments was shorter compared to neutral conditions, the duration was adequate for gastrointestinal absorption. Consequently, the NPSPHE@EOFAZ formulations developed are suitable for oral administration.
3.2 Cellular uptake
The biotoxicity of NPSPHE@EOFAZ was assessed through experiments conducted on Müller cells using the MTT viability assay (Fig. 2A-B). Three concentrations of EOFAZ (0.25, 0.5, and 1 µg/L) were selected based on prior laboratory investigations. Initially, the cytotoxic effects of EOFAZ and NPSPHE@EOFAZ on normal cells were examined across varying concentrations. Results depicted in Fig. 2A indicate that both EOFAZ and NPSPHE@EOFAZ exhibited no toxicity within the tested range of 0.25 to 1 µg/L.5 Subsequently, a HG concentration of 30 mM, as identified in previous research, was employed to induce cellular damage. As illustrated in Fig. 2B, Müller cells treated with HG demonstrated aberrant proliferation, which was mitigated upon treatment with EOFAZ and NPSPHE@EOFAZ. Notably, the cell viability at 1 µg/L EOFAZ was lower compared to 0.25 and 0.5 µg/L, leading to the selection of EOFAZ-L (0.25 µg/L), EOFAZ-M (0.5 µg/L), and NPSPHE@EOFAZ-L (EOFAZ: 0.25 µg/L) for subsequent assays.
The impact of NPSPHE@EOFAZ on HG-induced Müller cell morphology was assessed using the Giemsa assay (Fig. 2C). In the control group (Con group), cells exhibited elongated morphology with well-defined and evenly distributed intercellular spaces. Upon HG induction, cell proliferation increased, leading to blurred morphology and unclear intercellular spaces. Treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L resulted in amelioration of abnormal proliferation and morphology, with NPSPHE@EOFAZ-L demonstrating superior efficacy compared to EOFAZ-L in mitigating HG-induced Müller cell damage. These findings suggest that NPSPHE@EOFAZ suppresses abnormal proliferation and enhances the morphology of HG-induced Müller cells.
The water solubility of EOFAZ is limited, prompting its encapsulation into nanoparticles to enhance its solubility. The delivery of EOFAZ via nanomaterials was investigated using normal and HG-treated Müller cells. To facilitate tracking, FITC, a green fluorescent isothiocyanate, was linked to EOFAZ and NPSPHE@EOFAZ, yielding FITC-labeled EOFAZ and NPSPHE@EOFAZ. These compounds were then co-cultured with normal (Con) and HG-induced cells for 4 h. Mitochondrial fluorescent probes and DAPI were employed for mitochondria and nuclear staining, respectively. The results depicted in Fig. 2D-F reveal that NPSPHE@EOFAZ exhibited heightened green fluorescence in HG-treated cells, indicating enhanced drug uptake compared to other groups. Notably, NPSPHE@EOFAZ demonstrated superior green fluorescence signals relative to the EOFAZ group in both normal and HG-induced cells, underscoring its targeted drug delivery capability. Furthermore, NPSPHE@EOFAZ exhibited increased cellular uptake in HG-induced cells compared to normal cells. Under HG conditions, Müller cells exhibit elevated oxidative stress levels, leading to heightened cytomembrane permeability that facilitates cellular drug internalization.33 Conversely, EOFAZ, being hydrophobic with poor solubility, hinders cellular uptake. In contrast, nanoparticles show promise in improving the cellular uptake of hydrophobic drugs.15 Consequently, the incorporation of EOFAZ into NPSPHE resulted in enhanced cellular uptake owing to the superior drug delivery capacity of the nanoparticles.
3.3 ROS measurement
Müller cells, the primary glial cells spanning the entire retinal layer, normally play a role in glycogen synthesis and storage, providing nourishment to retinal neurons.34–36 However, underHG conditions, Müller cells become activated, leading to the generation of oxidative stress and inflammation.37–38 Initially, in the early stages of HG, Müller cells produce oxidative stress, triggering the expression of various inflammatory factors. Prolonged HG exposure results in the excessive buildup of ROS in the retinas of DR patients, causing damage to retinal endothelial cells and eventual vision loss.39–40 The accumulation of ROS, coupled with their inadequate clearance, may represent an irreversible factor in DR progression.41 Therefore, reducing oxidative stress in HG-induced Müller cells is crucial. For instance, Tu et al. demonstrated that melatonin activates the Sirt1 pathway, mitigating oxidative stress and inflammation in Müller cells during DR, thereby safeguarding the retina against diabetes-induced harm.1 To this end, NPSPHE, comprising a ROS-responsive PBE core, is engineered to selectively release drugs within environments of heightened oxidative stress.
To assess the ROS responsiveness of NPSPHE, it was co-incubated with an H2O2 medium, and the absorbance was measured at 600 nm using a UV spectrometer. The OD600 value and turbidity of the NPSPHE suspension decreased over time after H2O2 treatment, as depicted in Fig. 3A-B, indicating its sensitivity to ROS. ROS levels in HG-induced Müller cells were determined using the DCFH-DA probe. Following a 4-h co-culture of EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L with normal and HG-induced cells, DCFH-DA dye was utilized for cell staining, with results presented in Figs. 3C-D. In normal cells, no significant change in intracellular green fluorescence signal was observed with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L, suggesting no alteration in intracellular oxidative stress. Conversely, HG-induced cells exhibited elevated green fluorescence intensity, indicating increased ROS levels. Treatment with EOFAZ-L, EOFAZ-M, and NPSPHE@EOFAZ-L led to decreased green fluorescence intensity in HG-induced cells, signifying reduced cellular ROS levels. NPSPHE@EOFAZ-L demonstrated superior efficacy in alleviating oxidative stress compared to EOFAZ-L. The impact of EOFAZ and NPSPHE@EOFAZ on HG-induced intracellular oxidative stress was further evaluated through MDA and SOD assays (Fig. 3E-F). HG-induced cells displayed elevated MDA and decreased SOD levels compared to normal cells, indicative of heightened oxidative stress. Treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L resulted in decreased MDA levels and increased SOD levels in HG-induced cells, reflecting reduced oxidative stress. NPSPHE@EOFAZ-L exhibited better performance in reducing oxidative stress compared to EOFAZ-L, albeit inferior to EOFAZ-M.
The excessive production of ROS triggers the generation of inflammatory mediators and causes cellular damage, establishing a detrimental cycle in the retinal vasculature. To explore the inflammatory response, cell culture media were collected post-treatment with EOFAZ and NPSPHE@EOFAZ. Levels of IL-6 and IL-1β were quantified using ELISA kits as per the manufacturer's instructions. Results depicted in Fig. 3G-H illustrated elevated IL-6 and IL-1β levels in HG-induced Müller cells, indicating heightened inflammatory activity. Conversely, treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L led to decreased IL-6 and IL-1β levels, signifying potent anti-inflammatory effects. Notably, NPSPHE@EOFAZ-L exhibited superior efficacy in mitigating inflammatory responses compared to EOFAZ-L. In summary, NPSPHE@EOFAZ-L demonstrated enhanced antioxidative and anti-inflammatory properties in HG-induced Müller cells relative to EOFAZ-L, likely attributed to improved bioavailability facilitated by nanoparticle-mediated delivery.
3.4 In vivo assays
Due to the toxicity of EOFAZ, mice were orally administered with EOFAZ and NPSPHE@EOFAZ. Ocular tissues, comprising the cornea, conjunctiva, and retina, possess unique properties that pose challenges for the effective delivery of orally administered drugs. The presence of protective barriers in the eye, including the corneal epithelium and the blood-ocular barrier, presents a significant obstacle.42 These barriers function to impede the penetration of potentially harmful substances into the eye. The role of ocular barriers is essential for maintaining eye health, yet it poses challenges for drug delivery into ocular tissues. Oral administration primarily targets systemic drug distribution rather than specific delivery to the eyes. Upon ingestion, drugs are absorbed in the gastrointestinal tract, enter the bloodstream, and distribute throughout the body. Consequently, drug levels reaching the eyes are often limited. This study utilized small animal in vivo imaging to investigate the distribution of NPSPHE@EOFAZ in mouse eyes. The results showed high concentrations of NPSPHE@EOFAZ at 3 h post-administration, gradually decreasing over time in eye tissues. NPSPHE@EOFAZ exhibited higher fluorescence intensity and longer retention compared to EOFAZ in the eyes at specified time points. Following oral administration for 6 h, the fluorescence intensity of EOFAZ-BODIPY in the eyeball decreased to 48% of the 3-h level, while NPSPHE@EOFAZ-BODIPY maintained a high intensity at 87%. Even after 12 h, although both EOFAZ-BODIPY and NPSPHE@EOFAZ-BODIPY fluorescence decreased significantly in ocular tissues, NPSPHE@EOFAZ-BODIPY still showed stronger fluorescence than EOFAZ-BODIPY. These findings suggest that NPSPHE@EOFAZ can be absorbed and circulated through the gastrointestinal tract, ultimately leading to increased drug accumulation and retention in eye tissues.
DR is a common microvascular complication associated with diabetes, characterized by the leakage and blockage of retinal micro-vessels due to the chronic and progressive nature of the disease. While patients may not initially experience visual impairment during the early stages of metabolic dysfunction and DR, the condition is irreversible, underscoring the critical need for effective treatments in its early phases. Therefore, research focusing on intervening in the early pathological progression of DR and assessing the efficacy of potential treatments is imperative. In this study, diabetic mice were raised for 8 weeks to induce early-stage DR. The investigation aimed to evaluate the impact of NPSPHE@EOFAZ on the early pathological processes of DR. Analysis, as depicted in Fig. 4A, revealed that the control group displayed intact retinal cell layers with a well-organized structure. Conversely, the DR group exhibited disorganized outer nuclear layer (ONL) and inner nuclear layer (INL) cells, indicative of early-stage DR. Following treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L, the ONL and INL cells demonstrated a more orderly arrangement, suggesting a mitigation of disease severity. Notably, NPSPHE@EOFAZ-L exhibited superior efficacy compared to EOFAZ-L in ameliorating DR damage. These findings indicate that NPSPHE@EOFAZ decelerated the pathological progression and improved the pathogenesis of early-stage DR.
The in vivo antioxidant capacity of NPSPHE@EOFAZ was assessed through MDA, GSH, and SOD assays (Fig. 4B-D). DR mice exhibited elevated MDA levels and reduced GSH and SOD levels, indicating heightened oxidative stress. Treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L resulted in decreased MDA levels and increased GSH and SOD levels, indicating a mitigation of oxidative stress. Levels of IL-6 and IL-1β, markers of inflammatory response, were measured using ELISA kits (Fig. 4E-F). DR mice displayed elevated IL-6 and IL-1β levels. Following treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L, IL-6 and IL-1β levels decreased, suggesting a reduction in inflammatory response. NPSPHE@EOFAZ-L demonstrated superior antioxidant and anti-inflammatory effects compared to EOFAZ. In summary, NPSPHE@EOFAZ ameliorated the early pathological progression of DR by alleviating oxidative stress and inflammatory response.
Diabetes, a metabolic disorder marked by elevated blood sugar levels, can lead to chronic damage and dysfunction in multiple tissues, including the eyes, kidneys, heart, blood vessels, and nerves.43 Fluorescence imaging in Figure S4 revealed significant accumulation of NPSPHE@EOFAZ in the heart, liver, spleen, lungs, and kidneys. Subsequently, H&E staining was employed to examine the pathological alterations in these primary tissues. As depicted in Fig. 6, severe pathological changes were evident in all tissues of DR mice, which were mitigated following treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L. In the cardiac tissue of DR mice, cardiac myocytes exhibited irregular and disordered arrangement, along with irregularly shaped nuclei and noticeable bleeding. Treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L led to an improvement in the arrangement and morphology of myocardial cells. In the hepatic tissue of DR mice, hepatocytes appeared swollen, with large vacuoles in the cytoplasm displacing the nucleus to one side. Following treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L, vacuoles decreased in size and lesion severity improved. In spleen images of DR mice, the distinction between white and red pulp was initially unclear. However, treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L led to a clearer boundary between the white and red pulp, indicating a positive impact on spleen structure. Analysis of lung tissue in DR mice revealed inflammatory cell infiltration, alveolar cavity expansion, and alveolar septa rupture. Treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L resulted in improved alveolar cavity expansion, reduced inflammatory cell infiltration, and significantly decreased alveolar septa rupture. Examination of kidney tissue in DR mice showed irregular and disordered arrangement of epithelial cells in renal tubules. Treatment with EOFAZ-L, EOFAZ-M, or NPSPHE@EOFAZ-L improved renal lesions, indicating a beneficial effect on kidney tissue. Notably, NPSPHE@EOFAZ-L exhibited superior improvement in primary tissue damage compared to EOFAZ-L, and comparable results to EOFAZ-M. In conclusion, NPSPHE@EOFAZ demonstrated efficacy in reducing damage and inflammatory response in the primary organs of DR mice.
{kind=link}