Study design
This study is a multicenter, parallel, prospective, double-blind, randomized, placebo-controlled clinical trial. A total of 260 patients will be enrolled and randomly divided into the treatment and placebo groups. All patients will receive 10 consecutive days of treatment and follow up for 8 weeks. Efficacy and safety data will be collected truthfully throughout the study. Flowchart is Fig. 1.
Ethics
This trial has been successfully registered in the China Clinical Trial Registry (ChiCTR1900022902). Additionally, the study will be strictly conducted in accordance with the Helsinki Declaration, Good Clinical Practice (GCP) guidelines and laws. The research protocol, informed consent, and recruitment posters were reviewed and approved by the Ethics Committee of the Guangdong Provincial Hospital of Traditional Chinese Medicine (No. BF2018–180–01). The researchers in all six trial centers are well-trained and qualified medical staff. All eligible patients will be fully informed and totally understand about this protocol and will sign an informed consent form(ICF) prior to participation. All participants can receive all exams and treatments for free, and their privacy, data and security will be greatly protected.
Participants and recruitment
We will recruit patients who meet the criteria for inclusion by advertising on hospital notice boards, posting recruitment information in network communication groups or being recommended by outpatient and inpatient doctors. A total of 260 eligible participants will be recruited in the following 6 hospitals: (1) Guangdong Provincial Hospital of Traditional Chinese Medicine,(2) Guizhou Provincial Hospital of Traditional Chinese Medicine,(3) Second Affiliated Hospital of Guizhou University of Traditional Chinese Medicine, (4) Foshan Traditional Chinese Medicine Hospital,(5) Shenzhen longgang district hospital of traditional Chinese medicine,(6) Yangjiang people’s hospital. These six trial centers are all first-class hospitals in China, with advanced cardiovascular interventional departments, excellent medical teams and many inpatient beds. Especially the Guangdong Provincial Hospital of traditional Chinese medicine, which has the largest number of outpatients among hospitals of TCM in China, has rich experience and achievements in the research of integrated Chinese and western medicine.So the first center will be recruited 80 patients, and 36 at each of the remaining centers.
Inclusion criteria
For inclusion, participants should fulfill all the following criteria:
- Diagnosis of CMVD according to the 2017 edition of Chinese expert consensus on diagnosis and treatment of coronary microvascular diseases [11]
- Aged between 35 and 75, regardless of gender
- Willingness to participate and to sign the informed consent form,with high compliance and cooperative attitude.
Exclusion criteria
Participants with any of the following conditions will be excluded:
- Psychopaths,pregnant or lactating women;
- Patients with myocardial infarction,heart failure,stroke,arterial dissection,arterial embolization,tumors, severe hematologic diseases,endocrine diseases or pneumonia and other infections;
- Patients with liver and kidney dysfunction.( Expression of aminotransferase [ALT] and aspartate aminotransferase [AST] was 1.5 times higher than higher than the normal upper limit, abnormal serum creatinine,positive urine protein qualitative test)
- Patients with allergic to Guhong injection.
- Participated in other clinical trials and took actual experimental drugs within 3 months
- Patients who are not considered to meet the criteria by the researchers
Withdrawal criteria
The withdrawal criteria include the following:
- Experiencing serious complications or rapid deterioration of the condition during the trial, including angina attack frequency increased significantly,myocardial ischemia continued to worsen,myocardial infarction, arrhythmia and other changes.
- Serious adverse events occurred, which should be stopped according to the doctor’s judgment.
- Participants with important deviations in the implementation of the program, such as poor compliance and difficulty in evaluating drug effects.
- Quitting the clinical trial voluntarily.
Randomization and blinding
A total of 260 patients were randomly assigned according to the Numbers generated by the random number table. The singular one will be added to the Guhong group and the treatment of Guhong injection was noted on paper, the even one will be added to the control group and the 250ml placebo of 0.9% sodium chloride injection was noted, and then all papers were put into opaque envelopes,sealed and mixed evenly, and distributed to each trial centers. After the inclusion of patients, the envelopes will be opened successively by those researchers who did not participate in the recruitment, recommendation, data collection, evaluation and statistical work, and the patients were randomly assigned to the control group or Guhong injection group according to corresponding Numbers, and followed the instructions of notes on the paper for treatment.
Interventions
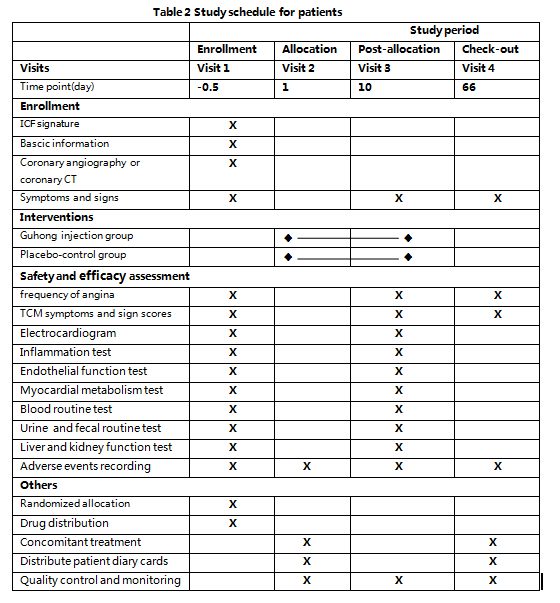
On the basis of conventional western medicine treatment, the Guhong group will be given 20ml intravenous infusion of Guhong injection which was diluted with 250ml 0.9% sodium chloride injection once a day, while the control group will be given 250ml 0.9% sodium chloride injection as placebo treatment once a day. (Guhong injection is provided by China tonghua guhong pharmaceutical co.LTD.The production batch number is 20190306 and each bottle has a capacity of 5ml. The drug distributed to each center will be labeled with the statement of”for trial only” and the information of name, dosage, dosing plan, indications, storage conditions, expiration date,manufacturer and so on. Each center has an independent manager responsible for receiving, handling, storing and distributing medications.)The course of treatment was 10 days. On the day of enrollment and at the end of treatment, the clinical symptoms and signs will be recorded, the quantitative table of TCM syndromes will be scored, the electrocardiogram will be examined, and the indicators of inflammation, endothelial function, myocardial metabolites and related biochemical tests will be conducted. Moreover, patients will be followed up for 8 weeks after the end of treatment, including the clinical symptom improvement and TCM syndrome quantitative score. During the entire study period, participants will be visited a total of 4 times by investigators. Specific research process details are provided in Table. 2.
Concomitant treatments and forbidden drugs
During the study period,participants with other diseases are allowed to continue corresponding treatment of western medicine, such as hypertension, diabetes, hyperlipidemia,et al.And the name, dosage and duration of any concomitant medication must be carefully recorded in the case report form (CRF), and any other western medicine or Chinese patent medicine that may affect the research results will be prohibited. Once banned drugs are used, patients will be dropped out of the study.
Efficacy assessment
Primary outcome
The primary outcome is the frequency of angina pectoris from the first day of enrollment to the end of treatment and at 8 weeks of follow-up.Each participant will be instructed to record any change in symptoms in their patient diary.
Secondary outcomes
Secondary outcomes include change in TCM symptoms and sign scores, change in ecg, therapeutic efficiency, change in the indicators of inflammation、endothelial function and myocardial metabolism.
Change in TCM symptoms and sign scores
The TCM symptom scoring system used in the study follows the Guidelines of clinical research on the treatment of coronary heart disease (chest pain) with New Chinese Medicine [12], in which all symptoms and scores are graded (Table 3). A total of 9 kinds of symptoms include: chest pain, chest tightness, breathless, palpitations, mental fatigue, aversion to cold and cold limbs, lumbar and knee soreness, spontaneous sweating and insomnia.The score is 0 point for asymptomatic, 1 point for mild, 2 point for moderate, and 3 point for severe. The total score ranged from 0 to 27. The lower the score, the milder the symptoms.
Therapeutic efficiency
The criteria for therapeutic efficiency evaluation is based on the principles for clinical research reports on cardiovascular drugs formulated by the National Health and Pharmaceutical Bureau of China [13] by comparing the angina attack frequency and ecg changes before and after treatment in the two groups of participants. Specific evaluation criteria are as follows:Significant effect: symptoms disappeared or significantly improved, angina attacks decreased by 80%, ecg returned to normal or generally normal; Effective: symptoms improved or the frequency of angina pectoris attacks decreased by 50–80%, the descending ST segment of the ecg rose ≥0.05mV, and the ascending ST segment fell ≥0.05mV, but still did not return to normal;,or the T-wave of the main ecg lead changed from flat to upright, or the T-wave changed from inverted to shallow by more than 50%; No effect: no change or even aggravation of clinical symptoms, no decrease or even increase of the frequency of angina pectoris attacks,no change or even aggravation of ecg ST-T.
Indicators of inflammation, endothelial function and myocardial metabolism
Indicators of inflammation, endothelial function and myocardial metabolism of participants before and after treatment will be tested in this study. Inflammatory indicators include hypersensitive c-reactive protein (hs-CRP), interleukin–6(IL–6)、Tumor necrosis factor-alpha(TNF-α). Endothelial function indexes include nitric oxide (NO) and endothelin–1 (ET–1)、Thromboxane A2 (TXA2). Myocardial metabolism indicators include cardiac troponin I (cTn Ⅰ), creatine kinase isoenzyme (CK - MB). Inflammatory reaction plays a significant role in the occurrence and development of coronary heart disease angina pectoris. TNF-α is the initiation factor of inflammatory response, which stimulates the synthesis and release of pro-inflammatory response factors (IL–6 and CRP), leading to the aggravation of inflammatory response and the formation of thrombus.[14、15] NO and ET–1 are the two most important vasoactive factors and the sensitive indicator of endothelial dysfunction in human body[16], NO can relax blood vessels [17], while ET–1 can promote vasoconstriction [18]. After vascular endothelial injury,TXA2 will promote platelet aggregation and vasoconstriction.[19] As for c Tn I and CKMB, they are ideal metabolites for early myocardial injury [20].
Safety evaluation
Liver and kidney function, blood routine, urine routine, fecal routine and electrocardiogram before and after treatment will be detected to assess the drug safety and adverse reactions.
Data management and statistical analysis
The drug clinical research center of guangzhou university of TCM will be responsible for the data statistical analysis. Two independent data administrators are in charge of reading the CRFs and recording data on the EpiData 3.1 software. And Clinical research assistants (CRA) and investigators will re-check and review the accuracy and consistency of data.After entering and reviewing, the database will be locked and the statistical analysis will be performed only with the permission of the sponsor, the principal investigator and the investigators.
The full analysis set (FAS) is the primary analysis set, in which patients should be dosed with Guhong injection or placebo for 10days with clinical observation record in the study. All subjects without any major protocol deviations will be included in the per-protocol set (PPS). Efficacy assessment will be performed through FAS and PPS. Safety evaluation will be conducted for those who have been treated at least once, which is defined as the safety set (SS).
All continuous data and normal distribution data are represented by mean ± standard deviation, while median and range for non-normal data. Classified data are expressed in frequency counts and percentages. Baseline balance between groups will be determined by chi-square test or anova. All the indicator obout angina attack frequency, inflammation, endothelial function and myocardial metabolites will be estimated and compared by the log-rank test. A Kaplan-meier survival curves will be constructed,and the median time will be provided separately for each group with a two-sided95% confidence interval. Analysis of variance (ANOVA) and Bonferroni method will be used to compare the TCM symptom and sign scores of the two groups. All collected data will be processed by professional statisticians using SAS 9.2 software; a two-sided P value of <0.05 is considered statistically significant
Quality control and monitoring
All case report forms (CRFs) are designed in strict accordance with relevant requirements of GCP,which be filled out by trained researchers to ensure consistency and reduce bias. If there is any ambiguity in the completion process, the results will be determined by the team members of the whole center after discussion. Each trial center has a project leader to control the quality, and all survey researchers are trained to be qualified and familiar with the process. In the process of clinical research, measures should be taken to ensure patient compliance according to the possible causes of shedding, and designated special cardiologists will visit each center regularly to check the original documents and CRFs, and supervise the study to ensure it complies with the protocol. Any shortcomings or problems found by inspectors should be improved.
{kind=link}