A thorough search and screening strategy was followed using PUBMED, SCOPUS, EMBASE, Web of Science, Google Scholar. The following terms were used for database search – ‘Obesity’, ‘bariatric surgery’, ‘Treatment’, ‘Obese’, ‘postoperative complication’, ‘quality of life’, ‘cost effectiveness’. A database was created with the search results and duplicates were removed. Included criteria were- Systematic Reviews, Meta-analyses, Narrative reviews, Observational Studies, Case reports and Case series. Articles that are in English were included with no limit on the date till Match, 2024. Editorials, short communications, letters to the editor, articles not focusing on bariatric surgery were excluded. Articles where the study population was not human and full text unavailable were also excluded. Articles were evaluated thoroughly for high quality evidence by the 4 authors and 53 eligible articles were finally included. Data was extracted from each study and assessed by two independent investigators using predefined Google sheets forms. The findings of the included studies were integrated and presented in a cohesive and narrative manner.
Bariatric treatment and procedure
Bariatric surgery is a type of surgery performed to help people with obesity lose weight and improve health problems associated with obesity. (8) Bariatric surgery involves multiple procedures, which include reducing the size of the stomach and providing alternative routes for food to pass through the stomach. (2) It is a safe, minimal risk option for people struggling to lose weight improving health problems like diabetes and increases lifespan.
The American Society of Metabolic and Bariatric Surgery (ASMBS) has established guidelines for the eligibility of metabolic and bariatric surgery. It is recommended for individuals with body mass index (BMI) > 35; or in patients with type 2 diabetes mellitus, BMI > 30. (8) Additionally, it is recommended for individuals with BMI 30-34.9 who fail to reduce weight or improve comorbidities using non-surgical methods.(8) It can also be an option for obese children and teenagers in some cases. Compared to traditional weight management care, which includes diet and exercise, bariatric surgery has proven to be more effective. (9) In a study comparing the two, the surgery group lost significantly more weight than the traditional group after several years. The surgery group did not regain the lost weight over time while the traditional group did. (9) Patients in the surgery group also saw a bigger improvement in health problems such as diabetes and hypertension compared to the traditional group.(9)
Bariatric surgery helps lose weight effectively and while the exact mechanisms are difficult to understand. (10) In particular, RYGB surgery improves blood glucose control in patients with type 2 diabetes compared to reducing calories through diet. RYGB speeds up the movement of nutrients through the small intestine, which leads to a large rise in blood glucose followed by a rapid drop. (11) This rapid change in blood glucose triggers the release of guy hormones, especially GLP-1, which reduces appetite and stimulates the release of insulin. Traditionally, weight loss mediated by bariatric surgery was thought to occur due to malabsorption. (12) However, malabsorption plays only a minor role in weight loss. Moreover, bariatric surgery stimulates the release of hormones, leading to changes in appetite and food preferences. (12) This is thought to occur due to changes in taste and smell sensitivity, which modifies caloric intake of patients and leads to weight loss.
Types of Bariatric surgery and WHO criteria for bariatric surgery
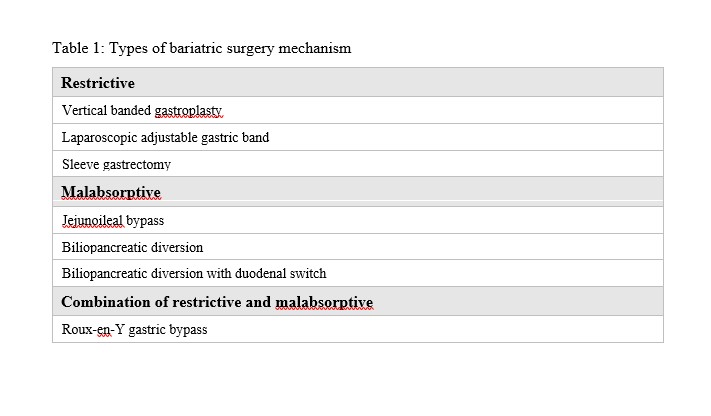
Bariatric surgery affects weight loss through three basic mechanisms: malabsorption, restriction, and the neurohormonal response that regulates hunger and energy balance. Some procedures have both a restrictive and a malabsorptive component. (Table-1)
Restrictive Procedures
Vertical Banded Gastroplasty shrinks stomach size by using both staples and a band to create a small gastric pouch. Food can enter the pouch and the
remainder of the stomach through a tiny opening in it.(13)
Globally, the most common bariatric surgery procedure is Laparoscopic adjustable gastric banding (LAGB). In LAGB, the stomach is physically reduced in size by placing an adjustable silicone band around it just below the gastroesophageal junction. This creates a pouch that has an initial volume of roughly 15ml. (13)
Originally performed as the initial stage of the duodenal switch treatment, sleeve gastrectomy (SG) is now performed as a stand-lone procedure, frequently using a laparoscopic method. By resecting the stomach’s greater curvature, the operation produces a tubular stomach with dimensions similar to that of a banana.(13)
Malabsorptive Procedures
The first surgical operation used to treat obesity was the jejuno-ileal bypass (JIB), which involves anastomosing the proximal jejunum to the terminal ileum. The jejuno-ileal bypass treatment has been discontinued due to its numerous severe side effects such as mineral, vitamin, and protein deficiencies, liver and renal failure, and even death. (14)
Biliopancreatic diversion (BPD) procedure involves dividing the duodenum from the pylorus, removing the pylorus, and dividing the ileum. The distal ileum is then anastomosed to the stomach and the proximal ileum, with the output from the liver, pancreas, and duodenum (or biliopancreatic limb) anastomosed to the terminal ileum some 50 to 100 cm away from the ileocecal valve. (13)
The biliopancreatic diversion with duodenal switch (BPD/DS) is a variant of the biliopancreatic diversion (BPD). The BPD with a DS procedure involves creating a sleeve gastrectomy with preservation of the pylorus and creation of a Roux limb with a short common channel. (15)
Combination of restrictive and malabsorption
RYGB is a common and most frequently performed bariatric procedure that involves creating a small gastric pouch and attaching it to a shortened small intestine. This restriction of food intake combined with nutrient absorption in the common channel helps with significant weight loss. (13)
In 1992, the National Institutes of Health (NIH) established eligibility criteria for bariatric surgery; these are still the most commonly used criteria. The eligibility requirements state that a person must meet either a BMI threshold of 40 kg/m2 or, in case of high risk comorbidities like severe type 2 diabetes or cardiovascular risk factors, a BMI threshold of 35 to 40 kg/m2. Therefore, bariatric surgery is not an option for anyone with a BMI of 35 kg/m2 or less. (16)
New NICE guidelines now recommend that these groups of people should be offered a comprehensive assessment for bariatric surgery without the requirement for all non-surgical interventions to have been tried first, or for patients to already be under the management of a tier 3 service. (17)
Effects of bariatric surgery on:
A. Health and postoperative complications
Factors including current body-mass index (BMI), total weight loss, employment status, presence of comorbidities, age and time since surgery were associated with Health related quality of life postoperatively. (18)
The most common long-term complications after gastric banding include band slippage and erosion.(19) Deflation or removal of the band is often required. Internal hernia, adhesions and anastomotic stenosis are common causes of intestinal obstruction after gastric bypass surgery. (19) Hepatobiliary complications pose a particular challenge because of the altered anatomy. (19) Complications after laparoscopic adjustable gastric banding include stomal stenosis, malpositioned bands, pouch dilation, band slippage, perforation, gastric volvulus, intraluminal band erosion, and port- and band-related problems. (20) Revision surgery, high age, low BMI, large waist circumference, and dyspepsia or gastro-esophageal reflux disease were associated with an increased risk for severe postoperative complication. (21)
B. Quality of life
Bariatric surgery is a popular treatment option for obesity, enhancing the quality of life (QoL) of patients. Its significant physical health improvements include weight loss, improved mobility, reduced strain, and decreased obesity-related health issues. (22) This leads to improved social interactions, fostering a sense of belonging and satisfaction. Effective obesity management can lead to increased life expectancy, reducing health risks associated with obesity. (22) Preoperative screening and postoperative support protocols are crucial for addressing these challenges. A comprehensive review of 18 studies shows that bariatric treatment provides a persistent positive impact on QoL, especially in its physical component score. (23) Long-term QoL benefits persist over time, with patients experiencing improved QoL beyond five years post-surgery.(24) More research is needed to fully understand the long-term impact on mental health aspects of QoL. Overall, bariatric surgery is a vital treatment option for obesity patients, enhancing their overall QoL (24)
C. Psychological aspect
Bariatric surgery has been found to have positive effects on the psychological well-being of patients with obesity, with a recent study showing improvements in depressive symptoms and overall quality of life following surgery. (25) However, another study also reported that pre-existing depressive symptoms do not significantly impact long-term weight loss outcomes. (26) The psychological aspects of bariatric surgery are profound and multifaceted. Many patients also reported improvements in mood, self-esteem, and overall mental health, as well as conditions like depression and anxiety. (25) Bariatric surgery can act as a catalyst for positive behavioral changes, such as increased physical activity and healthier eating habits. However, some patients may struggle with the significant lifestyle changes required after surgery and healthcare providers should offer psychological support to help them navigate these challenges. (25, 26)
D. Cost effectiveness
Bariatric surgery has demonstrated remarkable effectiveness in addressing severe obesity, leading to substantial weight loss and improvement in comorbidities. (27) Despite the initial costs associated with surgical intervention, numerous studies have indicated significant long-term cost savings within healthcare systems. (28) These savings primarily stem from reduced healthcare utilization, including decreased hospitalizations and medication expenditures, as well as improved productivity and quality of life for patients. (29) Additionally, advancements in surgical techniques and perioperative care have contributed to enhanced outcomes and cost-effectiveness of bariatric procedures over time. (30) However, variations in healthcare delivery and patient populations necessitate ongoing research to optimize the economic value of bariatric surgery across different contexts. (31)
E. Social factors
Bariatric surgery has not only demonstrated significant physiological effects but has also been shown to profoundly impact various social factors in patients' lives. (32) Research indicates that post-surgery, individuals often experience improvements in interpersonal relationships, including enhanced family dynamics and social support networks. (33) Furthermore, bariatric surgery has been associated with positive changes in psychosocial well-being, such as reduced depression and improved body image perception. (34) These improvements can lead to greater social integration and participation in activities previously avoided due to weight-related stigma. (35) However, it's crucial to acknowledge that social outcomes following bariatric surgery can vary widely among individuals, influenced by factors such as preoperative psychosocial functioning and postoperative adherence to behavioral recommendations. (36)
Challenges in Bariatric Surgery
Bariatric surgery has emerged as an effective treatment option in treating severe obesity, offering patients the chance to shed significant weight and keep it off long-term. It also has the potential to alleviate or even eliminate obesity-related health problems and reduce the risk of mortality. (37) However, the path to success after bariatric surgery is not always smooth, as patients may encounter various hurdles along the way, including physical, mental, and social challenges.
A. Physical Challenges
From a physical standpoint, patients must be prepared to commit to a lifetime of healthy habits, such as closely following a strict diet to prevent complications and ensure the surgery's effectiveness. (37) For some individuals, an unhealthy relationship with food may persist or even manifest after the surgery. Struggling with eating behaviors can lead to complications and jeopardize the long-term success of the procedure. Nutritional concerns are another critical aspect of post-bariatric surgery care. All types of bariatric procedures alter the structure and function of the digestive system to some extent, which can make patients more vulnerable to nutritional deficiencies such as anemia, osteoporosis, and protein malnutrition.(38) It is essential to identify and address any pre-existing nutritional shortfalls, like vitamin D and iron deficiencies, before surgery.(38)
Even though patients often see impressive initial weight loss results, the risk of regaining weight is a real concern for many. (39) Weight regain following bariatric surgery is a complex problem, and researchers are still working to understand its prevalence, causes, and treatment options. (39) This can happen due to a combination of factors, such as behavioral, physiological, and metabolic changes. The inconsistencies in how weight regain is defined and reported in studies highlight the need for a more uniform approach to this issue. (40) Identifying factors that may predict weight regain, such as low blood sugar after surgery, is essential for creating personalized post-surgery care plans that minimize this risk.
B. Psychological Challenges
The mental and emotional aspects of bariatric surgery are also complex, with research emphasizing the need for thorough psychological evaluations before surgery and ongoing support to address any issues that may arise afterward. (41) Some patients may continue to struggle with unhealthy eating patterns or develop new ones, which can lead to complications and hinder long-term success. (32) Post operative depression is another serious concern after surgery, as the dramatic life changes and potential complications can contribute to its onset.
For some individuals, the current postoperative care model may not be sufficient to prevent weight regain after bariatric surgery.(42) These patients often perceive weight regain as a personal shortcoming, and the accompanying shame and self-blame can make them hesitant to reach out for professional help or social support. Consequently, it is crucial for healthcare professionals to adopt an empathetic and non-judgmental approach when working with these patients, creating a safe and supportive space that encourages them to seek the assistance they need to maintain their weight loss and overall health.(42)
Moreover, patients may have to contend with loose, excess skin after losing a substantial amount of weight, which can be uncomfortable and may require additional surgeries to remove. (38) Recent advancements have led to the development of scoring systems that can predict excess body weight loss and identify specific biomarkers associated with suboptimal weight loss following bariatric surgery.(43) These tools provide valuable insights into a patient's potential for success and can help guide personalized treatment plans.
In addition to these predictive measures, individualized counseling plays a crucial role in optimizing outcomes for bariatric surgery patients. (43) This tailored approach can assist in selecting the most appropriate surgical procedure, strengthening self-monitoring skills, enhancing motivation, and promoting mindful eating habits. By addressing these key factors, personalized counseling aims to reduce the risk of weight regain and ensure long-term success. (43) As the field of bariatric surgery continues to advance, more research is needed to develop better strategies for preventing weight regain and addressing the long-term effects of these procedures.
C. Social Challenges
Individuals who feel more supported by their social network tend to fare better after bariatric surgery, experiencing reduced symptoms of depression, fewer body image concerns, and more successful weight loss outcomes. (44) This crucial support can be derived from various sources, such as family members, friends, healthcare professionals, and support groups. Participating in support groups following bariatric surgery has been linked to greater weight loss success. (45)
However, access to bariatric surgery can be hindered by a range of demographic factors, including insurance coverage, socioeconomic status, language barriers, ethnicity, and gender. (46) For example, some ethnic groups may face a lower likelihood of undergoing bariatric surgery due to financial limitations or the specific type of insurance they possess.
Recognizing and tackling the social challenges associated with bariatric surgery is essential not only for optimizing individual outcomes but also for promoting fair and equitable access to this transformative procedure for all who could potentially benefit from it. By addressing these challenges, we can work towards ensuring that everyone who qualifies for and desires bariatric surgery has the opportunity to pursue this life-altering treatment, regardless of their background or circumstances.
{kind=link}