The use of automated and objective methods for quantifying hemorrhage volumes has the potential for improving the prediction of complications following aSAH compared to subjective grading scales. The Fisher scale only achieved moderate correlation with the objective quantification of hemorrhage, highlighting the poor performance of this subjective scale. Specific volume thresholds are more likely correlated with the occurrence of vasospasm, acute hydrocephalus, SDH, and mortality within seven days. Furthermore, our findings suggest a weak correlation between the size of the aneurysm and the volume of hemorrhage.
Hemorrhage volume post-aSAH has traditionally been assessed subjectively, leading to considerable interrater variability. Van der Gagt et al. observed significant variability in the assessment of hemorrhage volume on 159 aSAH CT scans (kappa 0.34–0.66).18 Similarly, Van Norden et al studied 132 aSAH CT scans and found that the interobserver agreement of the Fisher scale was only mild to moderate (kappa 0.37–0.55).19 New semiautomated9 and automated,10–13 methods have been used for hemorrhage volume quantification. A recent meta-analysis conducted by Matsoukas et al. encompassed 40 studies detailing artificial intelligence (AI) algorithms designed for intracranial hemorrhage detection.20 On average, most AI-driven software tools had a high performance for the diagnosis of intracerebral hemorrhage, however, specific thresholds for aSAH complications prediction were not reported.
Quantifying hemorrhage volume in aSAH poses challenges due to blood distribution across subarachnoid spaces, ventricles and parenchyma. Ziljstra et al.’s analysis of 333 patients using an automated detection method found intraventricular hemorrhage to be a predictor of delayed cerebral ischemia (DCI), while intraparenchymal hematoma showed a negative association.10 In contrast, Platz et al reported that intraparenchymal hemorrhage was associated with DCI.21 The precise factors leading to DCI remain unclear, but accurately measuring total intracerebral hemorrhage could better predict DCI and complications like symptomatic vasospasm, SDH, and poor functional outcomes following aSAH.22 Moreover, in the era of AI, defining blood volume thresholds may refine prognostic evaluations and enhance patient outcomes. In AUC analysis, an aSAH volume of 15 mL exhibited moderate accuracy in predicting symptomatic vasospasm (65.2% sensitivity and 60.1% specificity, AUC 0.65). In a smaller cohort of 42 patients, Street et al. reported that a semi-automated method outperform the modified Fisher scale in predicting radiological vasospasm, achieving a higher accuracy (AUC 0.86 vs 0.70).23 Variability in reported incidences of radiological vasospasm, symptomatic vasospasm, and DCI across studies highlights the lack of standardized definitions and outcomes in this research area.24
In our analysis, an aSAH volume of 9.95 mL achieved a higher accuracy for the occurrence of hydrocephalus (sensitivity of 74.2% and specificity of 69%). This volume is notably smaller than the volumes associated with vasospasm, and death within 7 days. Only a small volume of hemorrhage may be necessary to obstruct or damage the pathways responsible for CSF circulation and absorption. Hemorrhage volume is also pivotal in assessing the likelihood of SDH. A meta-analysis conducted by Wilson et al. on the risk factors associated with SDH revealed a strong correlation between the presence of intraventricular blood (OR 3.93) and SDH.25 We report a volume of 16.76 mL for predicting SDH post-aSAH (sensitivity of 64% and specificity of 60%). Previously, Garcia et al. studied a cohort of 168 patients using a manual method for hemorrhage assessment and reported a threshold of 10.3 mL for SDH. This threshold was less sensitive of (50%) but more specific (83%) than the threshold reported in our study.8 This disparity may be explained by the different clinical criteria in determining the need for a permanent shunt.
Mortality in the acute phase of aSAH can be the result of multiple factors, but a larger hemorrhage burden often plays a pivotal role. In our study, a volume of 33 mL of aSAH was very accurate in predicting mortality within 7 days (sensitivity of 79% and specificity of 76.9%). Similarly, Lagares et al. examined 206 patients and found that the proportion of individuals with poor outcomes, defined as Glasgow Outcome Scale score of 3 or lower, increased from 35% when the aSAH total hemorrhage volume was below 20 mL to 86% when it exceeded 20 mL.22
Aneurysm size and hemorrhage volume
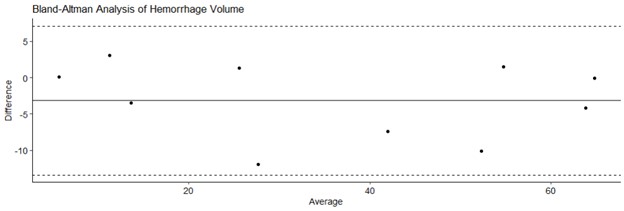
It is unclear whether larger aneurysms lead to larger hemorrhages. While it might seem logical to assume that a larger aneurysm could result in more significant bleeding, Wiebers et al. have suggested the possibility of aneurysms diminishing in size upon rupture.26 Our study found only a weak correlation between aneurysm size and hemorrhage volume (Fig. 2). This disparity may stem from the intricate combination of variables at play during aneurysm rupture, including blood pressure, the diameter of the parent artery, and the presence on adjacent structures such as brain parenchyma that would potentially constrain the amount of hemorrhage, among other factors.
This study has several limitations. Being a retrospective analysis of a large patient cohort, certain confounding factors that could influence clinical outcomes may not have been precisely accounted for. Consequently, our analysis concentrated on identifying symptomatic vasospasm rather than DCI, since the latter poses more challenges for retrospective determination. In contrast, vasospasm was objectively documented during hospitalization, making it a more reliable focus for our study.
{kind=link}