The prognosis following CCA resection hinges on several tumor-specific factors such as lymph node metastasis, differentiation, and resection-based curability[46]. However, most of these factors can only be ascertained post-operation. In clinical practice, prognostic factors identifiable before surgery prove more beneficial. Hence, we conducted a systematic review and meta-analysis of several studies to explore the relationship between various preoperative body composition indicators and the prognosis of CCA after radical surgery. Our study examined how sarcopenia, sarcopenic obesity, myosteatosis, and BMI relate to postoperative outcomes such as overall survival (OS), recurrence-free survival (RFS), as well as the occurrence of complications and recurrence. Because these factors can be determined before surgery, they play an important predictive role in guiding the post- operative prognosis of patients with cholangiocarcinoma.
Sarcopenia has been identified as a predictor of postoperative morbidity and mortality in liver transplantation, as well as in several other gastrointestinal cancers[47, 48]. Our results are consistent with these studies, showing that sarcopenia significantly reduces survival time (OS and RFS), increases the likelihood of major postoperative complications, and raises the risk of postoperative recurrence. The mechanisms underlying the association between sarcopenia or skeletal muscle wasting and morbidity and mortality remain incompletely understood. However, this connection may arise from malignancies triggering an excessive inflammatory response, leading to reduced energy and consequent muscle mass loss[49]. Research on the impact of sarcopenia on postoperative outcomes in CCA is highly significant. In an aging society, sarcopenia (SP), characterized by the age-related decline in skeletal muscle mass, strength, and physical performance[50], has been steadily increasing worldwide, with an overall prevalence ranging from 10–27%[51].
Recently, in addition to sarcopenia, there have been reports indicating that sarcopenic obesity is a significant prognostic factor for malignancy[52]. Previous study has revealed that muscle wasting in the presence of obesity may lead to even lower physiological reserves and an increased risk of perioperative morbidity and mortality[53]. Our findings indicate that evaluating the preoperative status of sarcopenic obesity in patients with CCA is essential, as it significantly diminishes both overall survival (OS) and recurrence-free survival (RFS), while also raising the probability of major postoperative complications.
Myosteatosis, defined by the infiltration of adipose tissue into muscle tissue[21], has been consistently linked to postoperative complications, prolonged hospital stays, and increased mortality rates in various gastrointestinal cancers[54]. Prior to our study, a recent investigation involving 75 palliative CCA cases highlighted the prognostic importance of both sarcopenia and myosteatosis, assessed using L3 CT SMI and SM-RA, albeit without distinguishing between CCA subtypes[55]. Our findings are consistent with these studies, indicating that myosteatosis significantly diminishes both overall survival (OS) and recurrence-free survival (RFS), along with elevating the risk of major postoperative complications.
When it comes to Body Mass Index, the situation becomes more complex. Kumamoto et al. found that BMI and the neutrophil-to-lymphocyte ratio (NLR) were significant predictors of postoperative complications[56]. A comprehensive retrospective study suggests a potential association between obesity and surgical wound infections as well as prolonged operative duration[57]. This partially aligns with our study findings. Our results indicate that patients with a BMI > 25, classified as overweight or obese, indeed have a higher incidence of major postoperative complications following CCA surgery. However, the overweight or obese condition does not worsen the postoperative overall survival (OS) and recurrence-free survival (RFS) for these patients. This may be attributed to the fact that, despite overweight or obesity leading to more complications, patients with this condition inherently possess a richer nutritional energy reserve, which is a favorable factor for surgery. Similarly, our study found that BMI < 20 does not worsen the postoperative overall survival (OS) and recurrence-free survival (RFS) for these patients. This may be because although these patients have fewer nutritional energy reserves, they may experience fewer postoperative complications.
Since body composition is associated with postoperative survival rates and the incidence of complications, perioperative intervention is crucial to mitigate the risks associated with unfavorable body composition conditions. Nutritional counseling and oral nutritional supplements are potential intervention options for addressing unfavorable body composition conditions, effectively reducing the occurrence of preoperative malnutrition. For instance, research indicates that preoperative exercise and nutritional support programs in patients with gastric cancer can lower the prevalence of sarcopenia and enhance postoperative outcomes[58]. It's important to recognize that assessing body composition should involve a variety of indicators. Beyond just BMI and obesity status, attention should also be given to factors like muscle mass. Therefore, highlighting the significance of identifying muscle wasting, which might be obscured by excess adipose tissue, can aid in selecting patients for prognosis and risk assessment. Additionally, it can facilitate therapeutic interventions such as nutritional counseling and support, as well as physical prehabilitation[59]. As a result, actively monitoring the body composition of CCA patients preparing for surgery and striving to improve the conditions of sarcopenia, sarcopenic obesity, and myosteatosis can greatly benefit their postoperative prognosis.
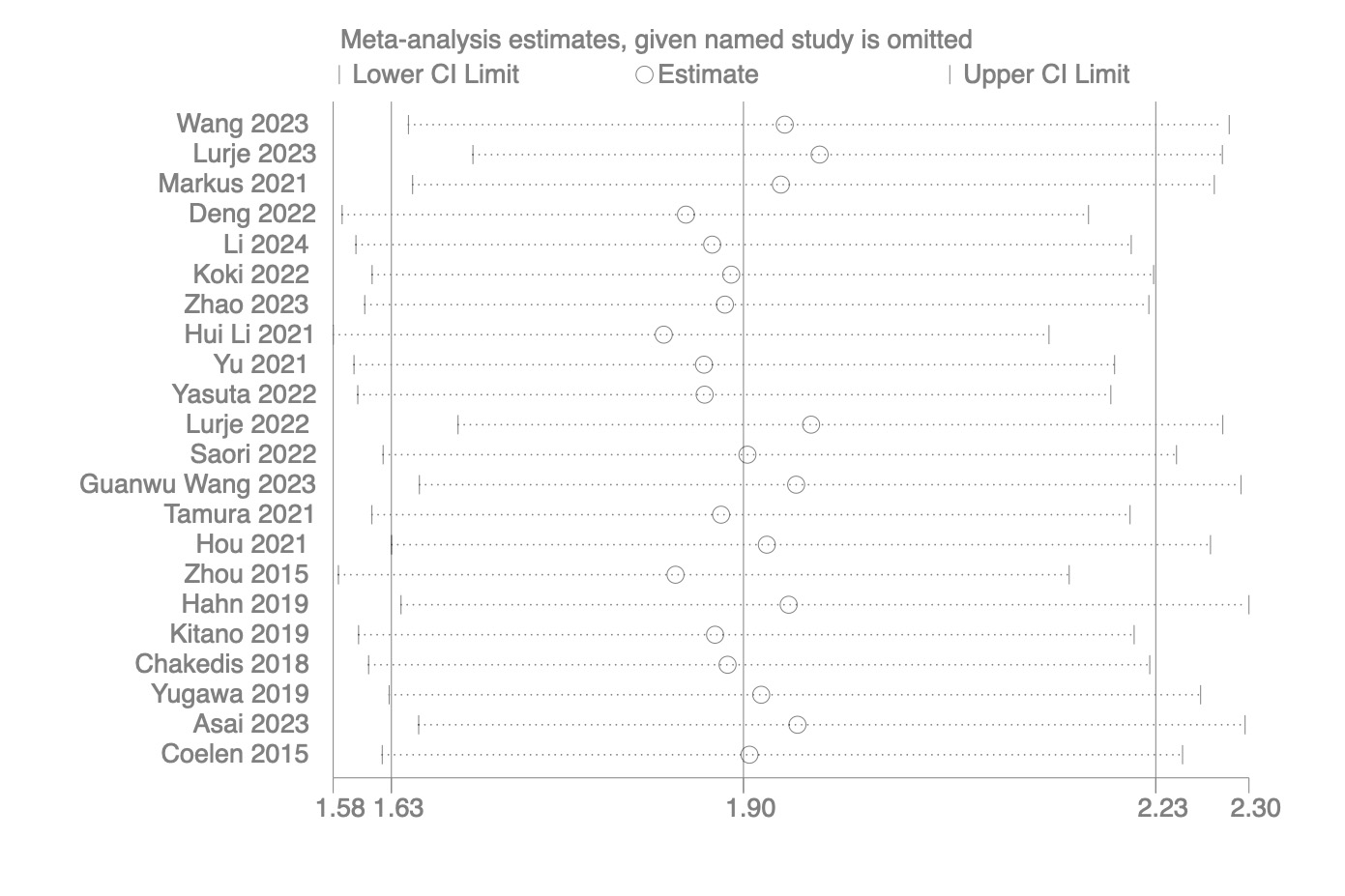
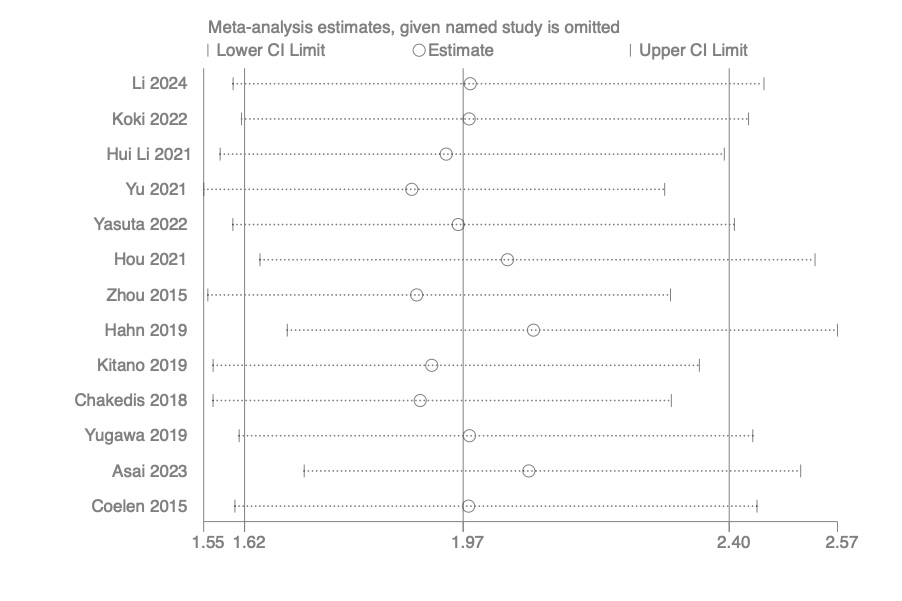
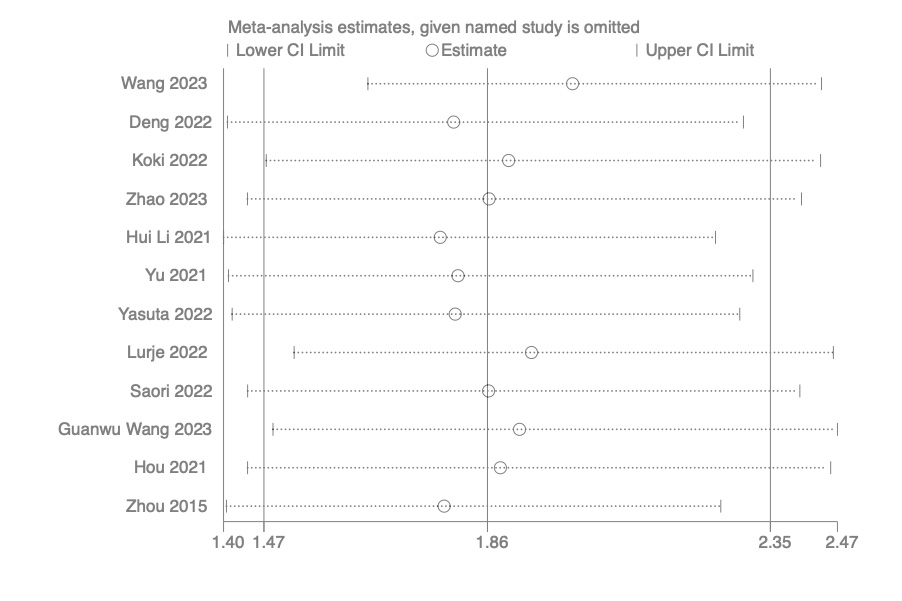
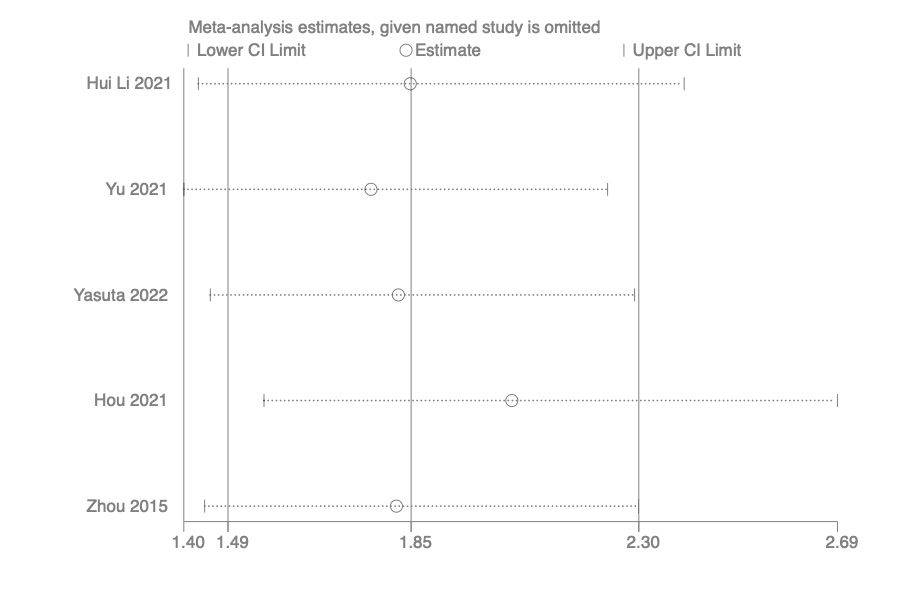
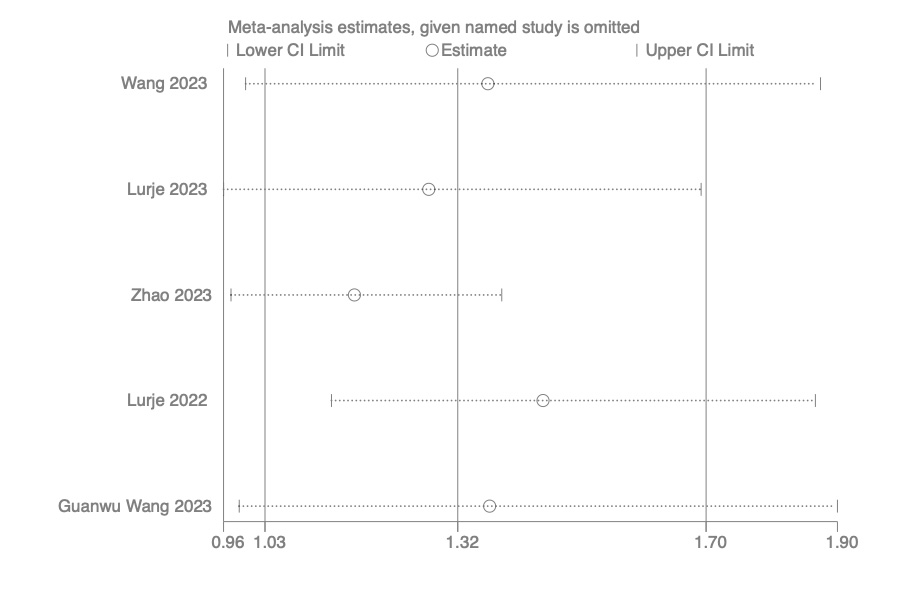
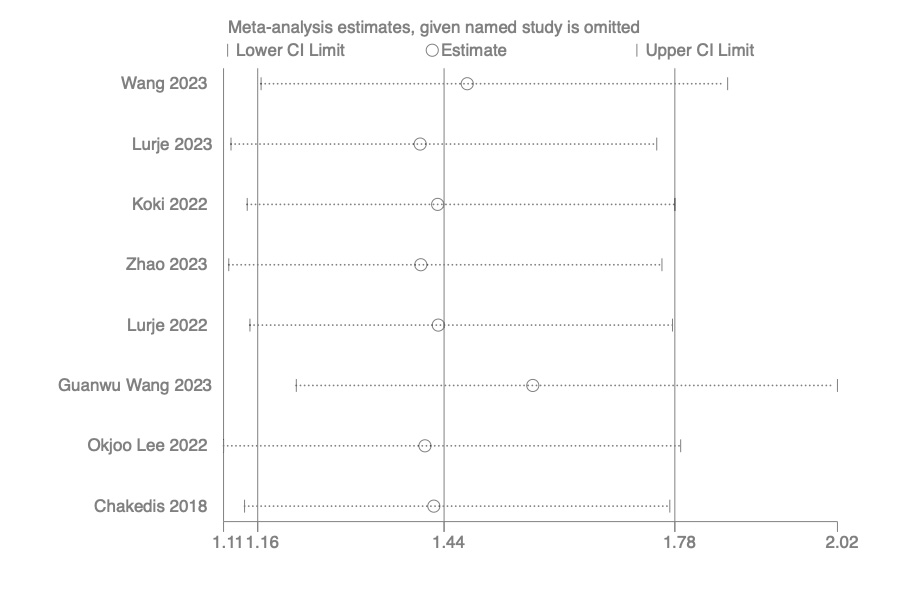
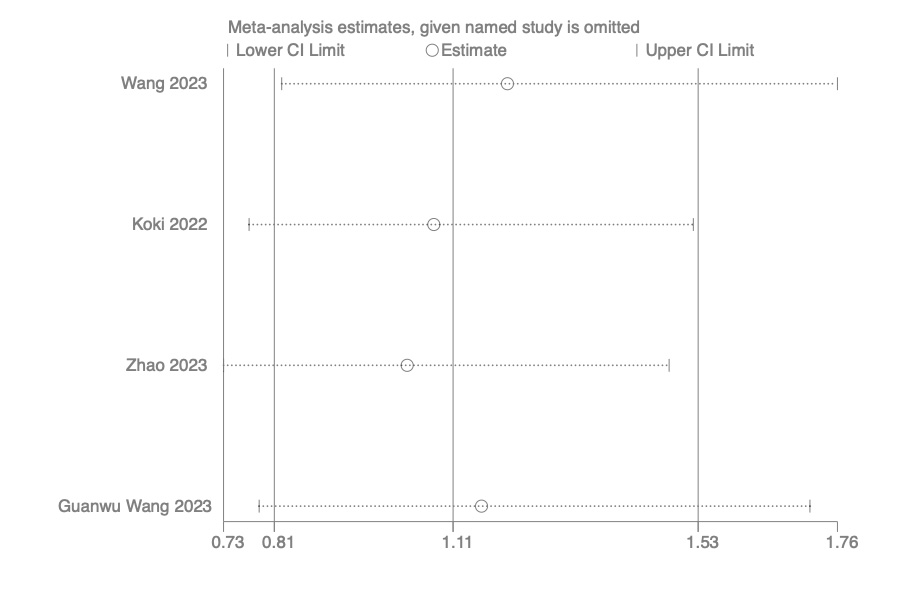
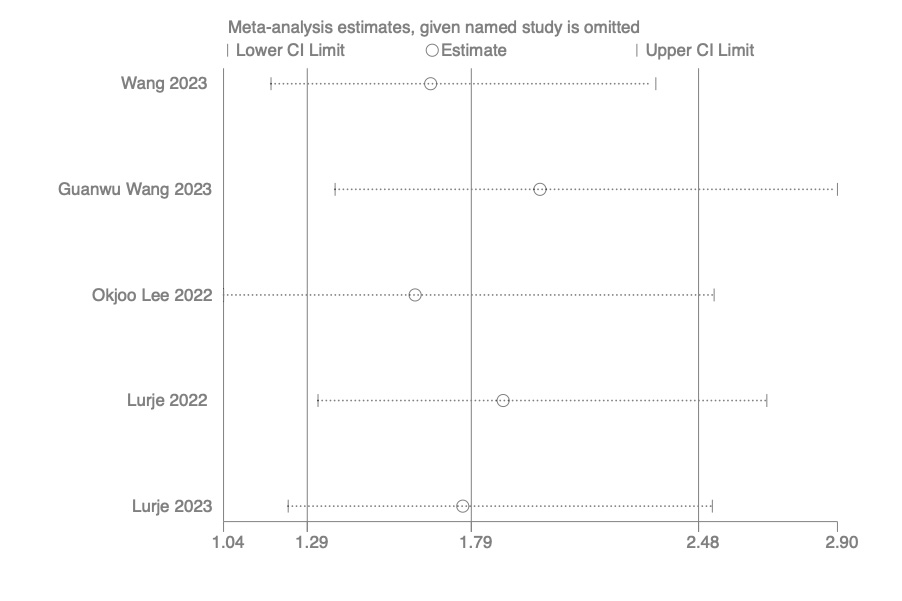
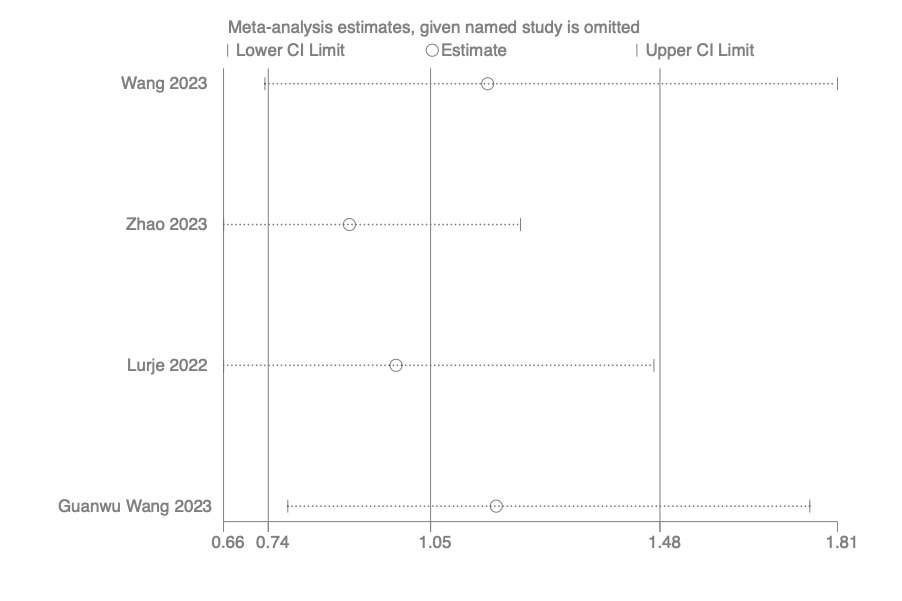
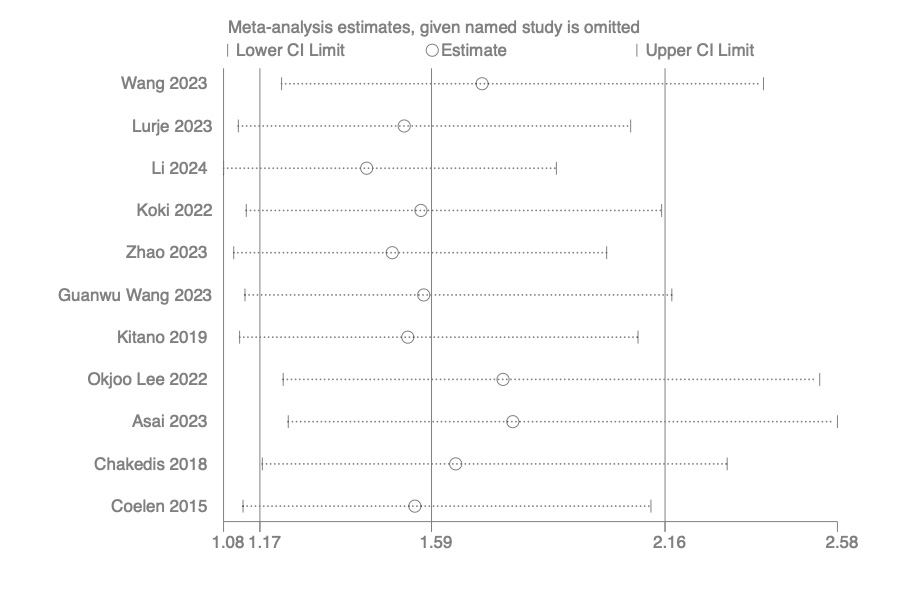
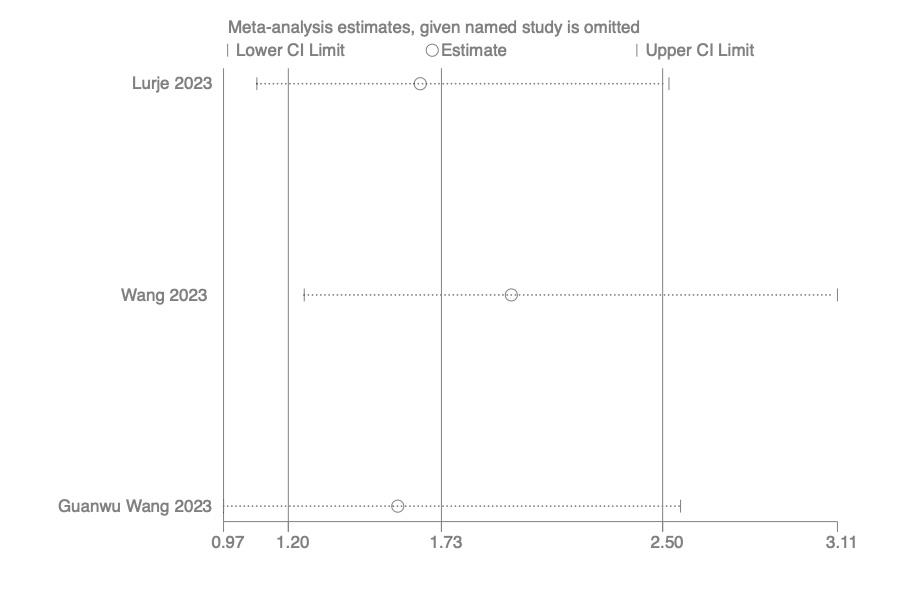
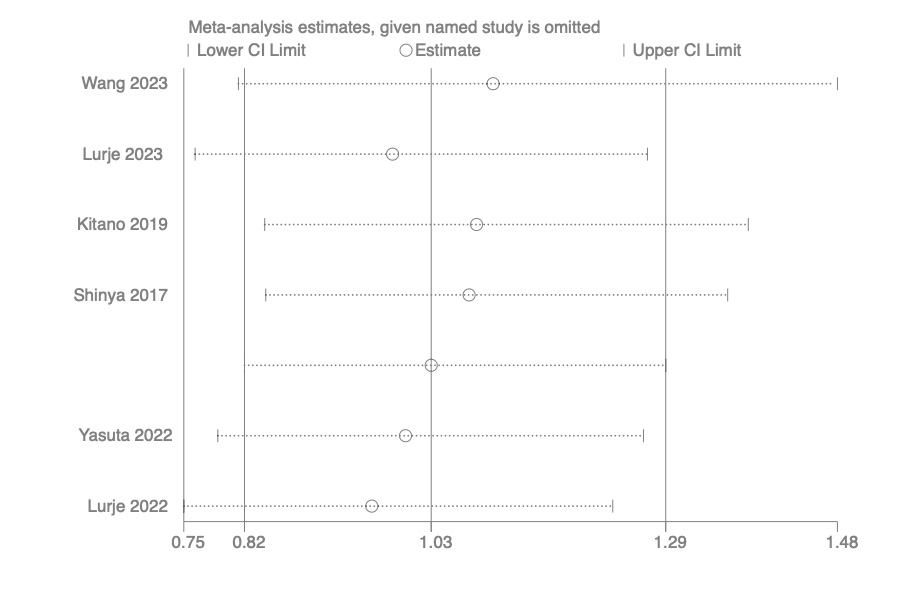
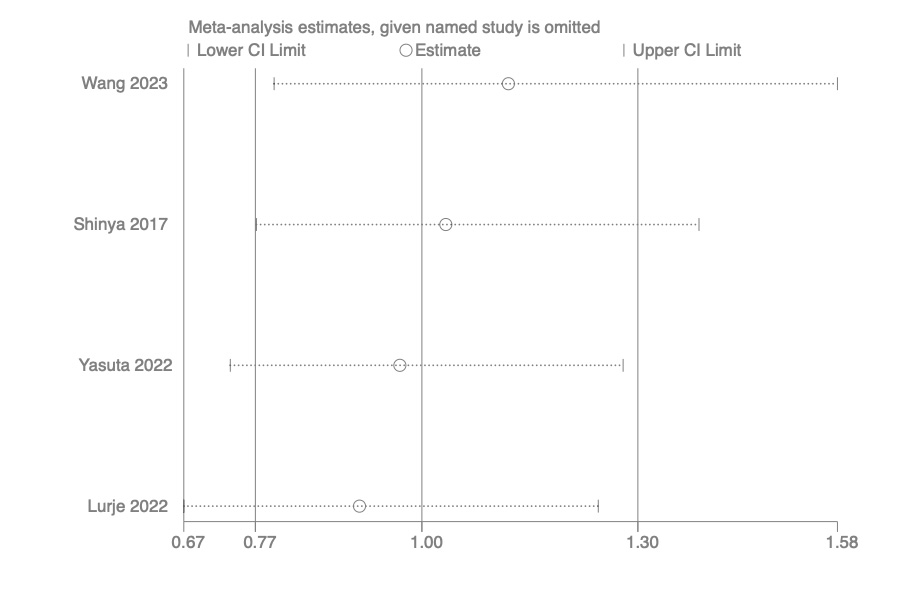
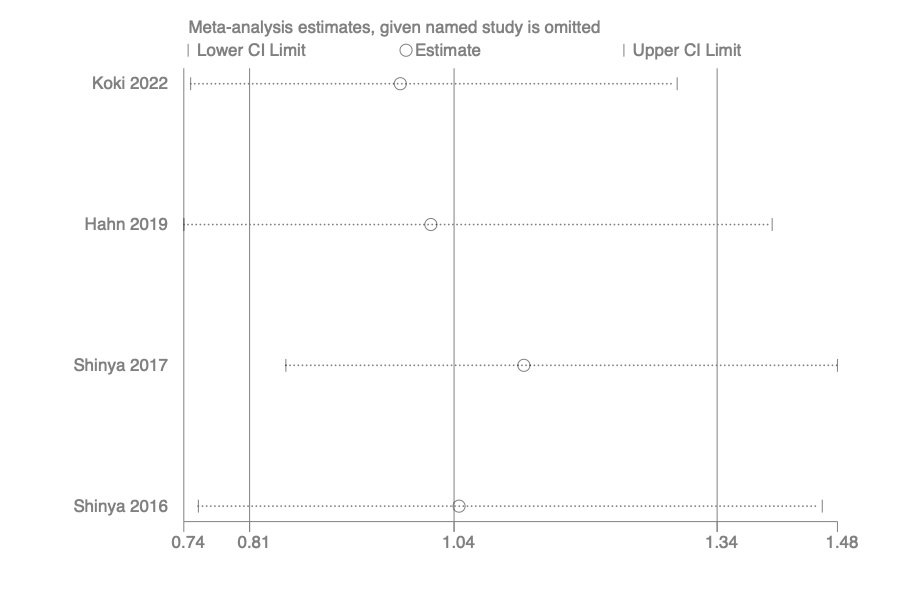
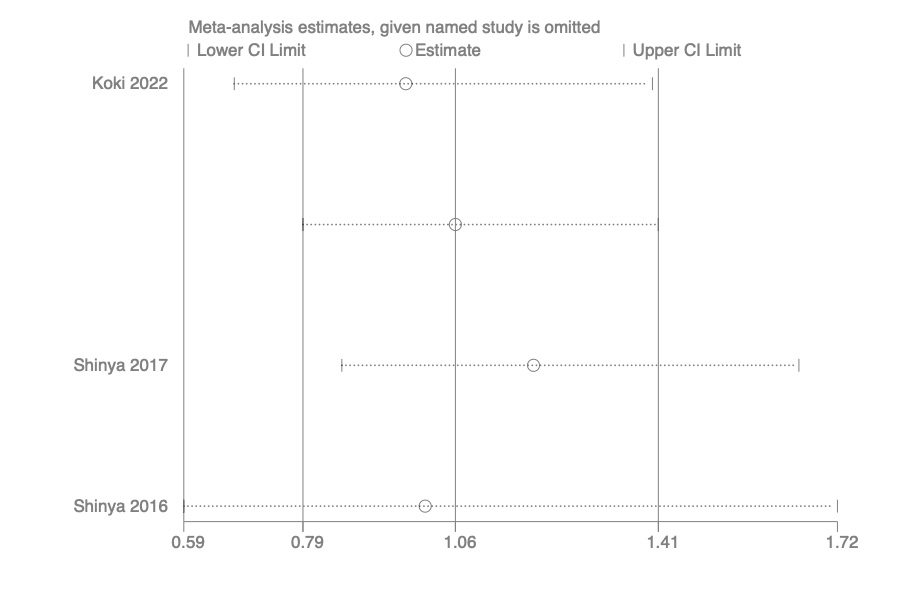
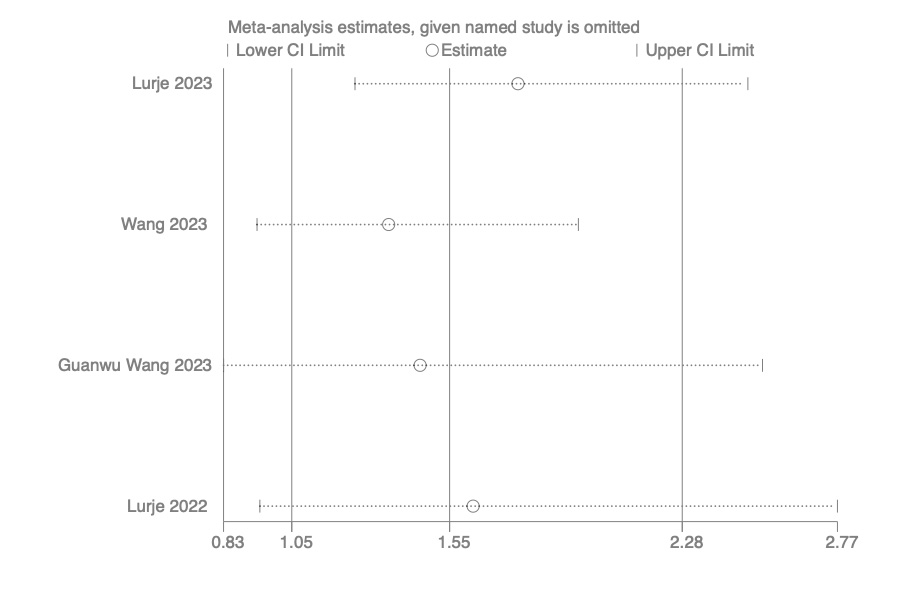
To explore the sources of heterogeneity, we conducted subgroup analyses, stratifying by the measurement methods of muscle mass (SMI or PMI) and the subtypes of cholangiocarcinoma categorized by anatomical structures (ICC, PCC, ECC). Our subgroup analyses based on different measurement methods of muscle mass and the subtypes of cholangiocarcinoma did not alter the overall results. We performed a thorough sensitivity analysis to ensure the reliability of our study findings. We conducted a thorough evaluation of potential publication bias and presented detailed Egger test results for each outcome.
We must acknowledge several limitations in our study. Firstly, all the included studies were retrospective cohort studies. Moving forward, large-scale randomized controlled trials are warranted to provide further insights into the relationship between body composition and the prognosis of CCA following surgery. Secondly, due to the limited number of primary studies, certain subgroup analyses could not be conducted. For example, the association between preoperative myosteatosis and DCC prognosis could not be assessed due to insufficient research on this relationship. Therefore, these relatively understudied aspects warrant further investigation in future research endeavors. Thirdly, some cutoff values for body composition are subject to debate. For instance, while the normal BMI range is considered to be 18.5 to 25, our study could only investigate the impact of BMI on prognosis using cutoffs of < 20 and > 25. This limitation stems from the constraints of the original studies' BMI cutoff values. However, to the best of our knowledge, this study represents the first meta-analysis to comprehensively examine the association between body composition and prognosis following radical resection of CCA. Furthermore, we conducted thorough subgroup analyses based on different measurement approaches for muscle mass and various tumor locations of CCA.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}