This study provides the first complete mapping of avoidable hospitalisations for ACSCs in Switzerland in 2017. Using small area analysis to determine regional variation for various ACSCs and primary care structures, we found substantial regional variation with distinct disease-specific regional patterns. Standardized for sex and age, the overall degree of regional variation was higher than in other European countries i.e. Denmark, England Portugal, Slovenia and Spain (36).
General characteristics
Our results suggest that 4.3% of all hospitalisations in 2017 were avoidable. Furthermore, we observed a gradual increase in avoidable hospitalisations for ACSCs in the population above 65 years of age, peaking at the 80-84-year age group. This pattern is consistent with results from a similar study that investigated avoidable hospitalisations for ACSCs in France (6).
More specifically, consistent with previous studies in Germany, we found that hospitalisations for congestive heart failure and COPD account for a substantial fraction of avoidable hospitalisations (7, 10). About half of the identified cases were referred to hospital by physicians, with roughly three quarters of patients admitted to hospital as emergencies.
Our sample’s Elixhauser comorbidity scores were rather high at 4.5 (IQR 4.0-5.0) compared to those measured by van Walraven et al. (2009), who recorded a median score of 0 (IQR 0-8). This indicates, that our population had more comorbidities present, than a regular hospital cohort. Aditionally, the high number of emergency admissions suggest that the admitted patients had experienced a profound deterioration of their already fragile health prior to admission with multiple comorbidities. Interestingly, about 30% of cases are readmitted to hospital within the year 2017, indicating challenges in primary health care provision, especially regarding self-management and monitoring of early warning signs.
When addressing overall unadjusted rates of avoidable hospitalisations for ACSCs, we found similar results for four of our diagnoses of interest (congestive heart failure, COPD, diabetes complications and hypertension) also used in a similar study by Berlin et al. (2014) in the Swiss context (2). Compared with that study’s findings, our overall unadjusted rates of avoidable hospitalisations for ACSCs indicate an increase of 2.7% over a seven year period (2). However, compared to similar studies in Swiss, French and German contexts (2, 6, 7), this increase is actually quite low.
Standardized rates of avoidable hospitalisations for ACSCs in Switzerland were high in the European context; likewise, regional variations for the ACSCs of interest were considerably higher in Switzerland than in other European countries (36).
Regional Variation
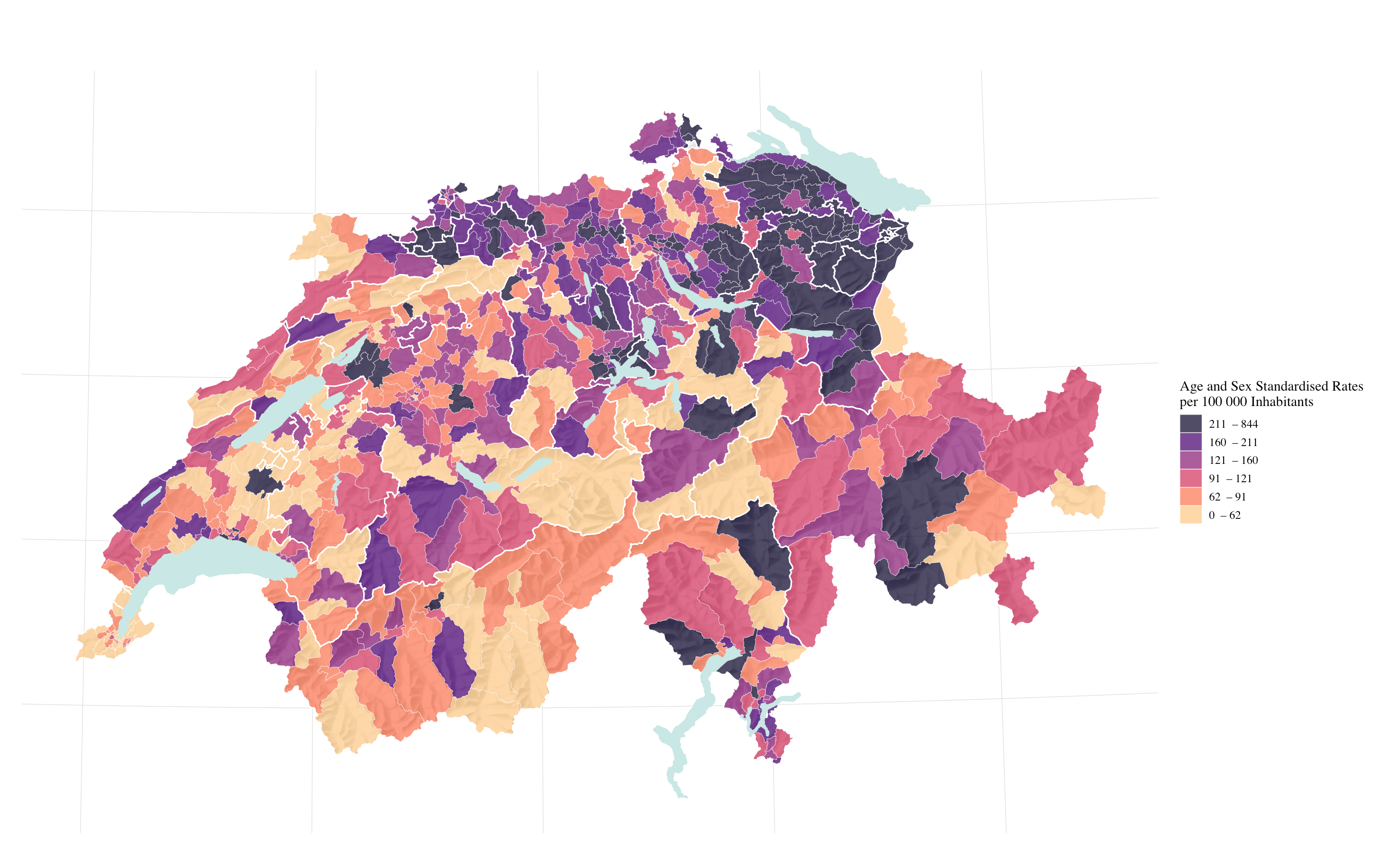
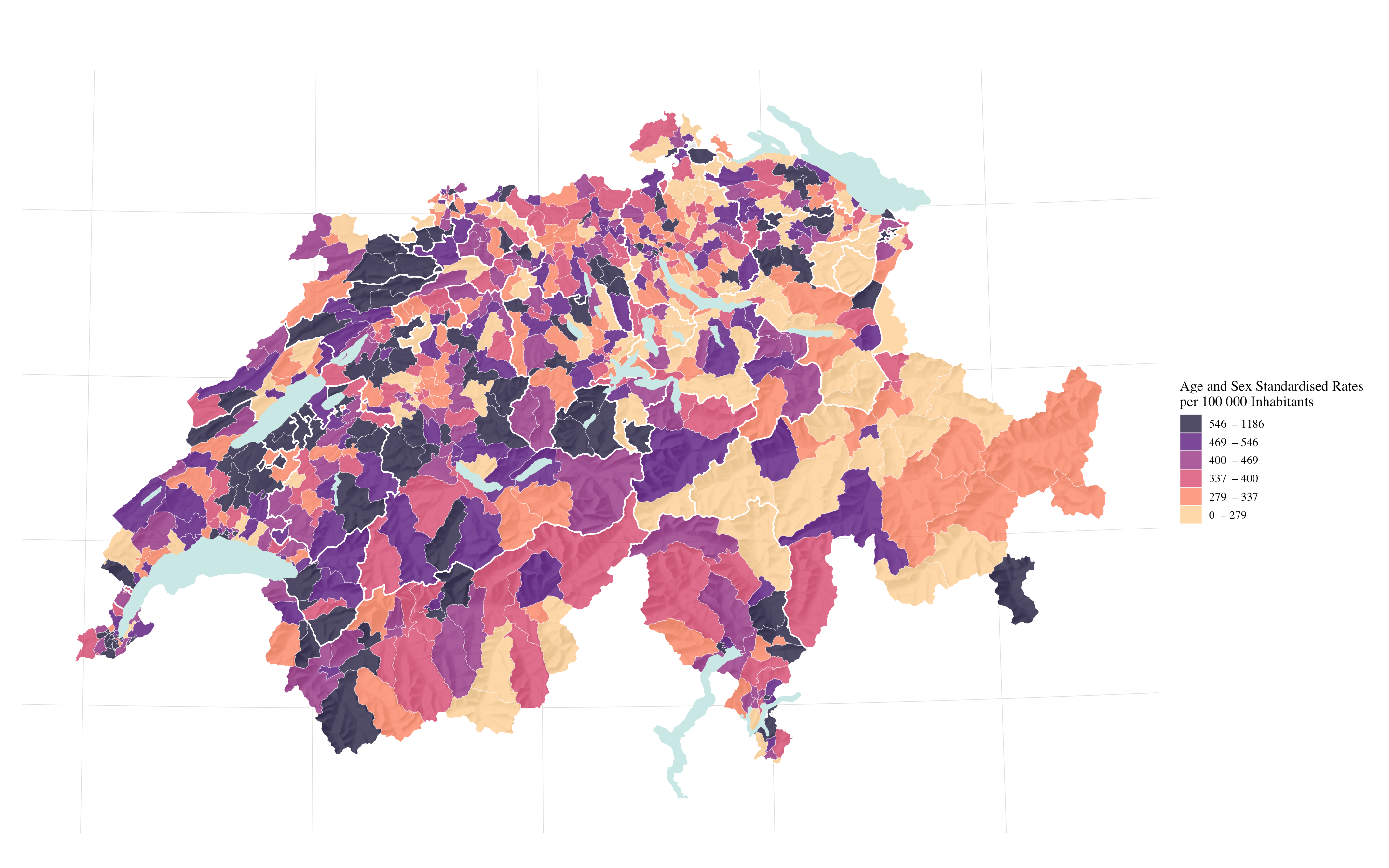
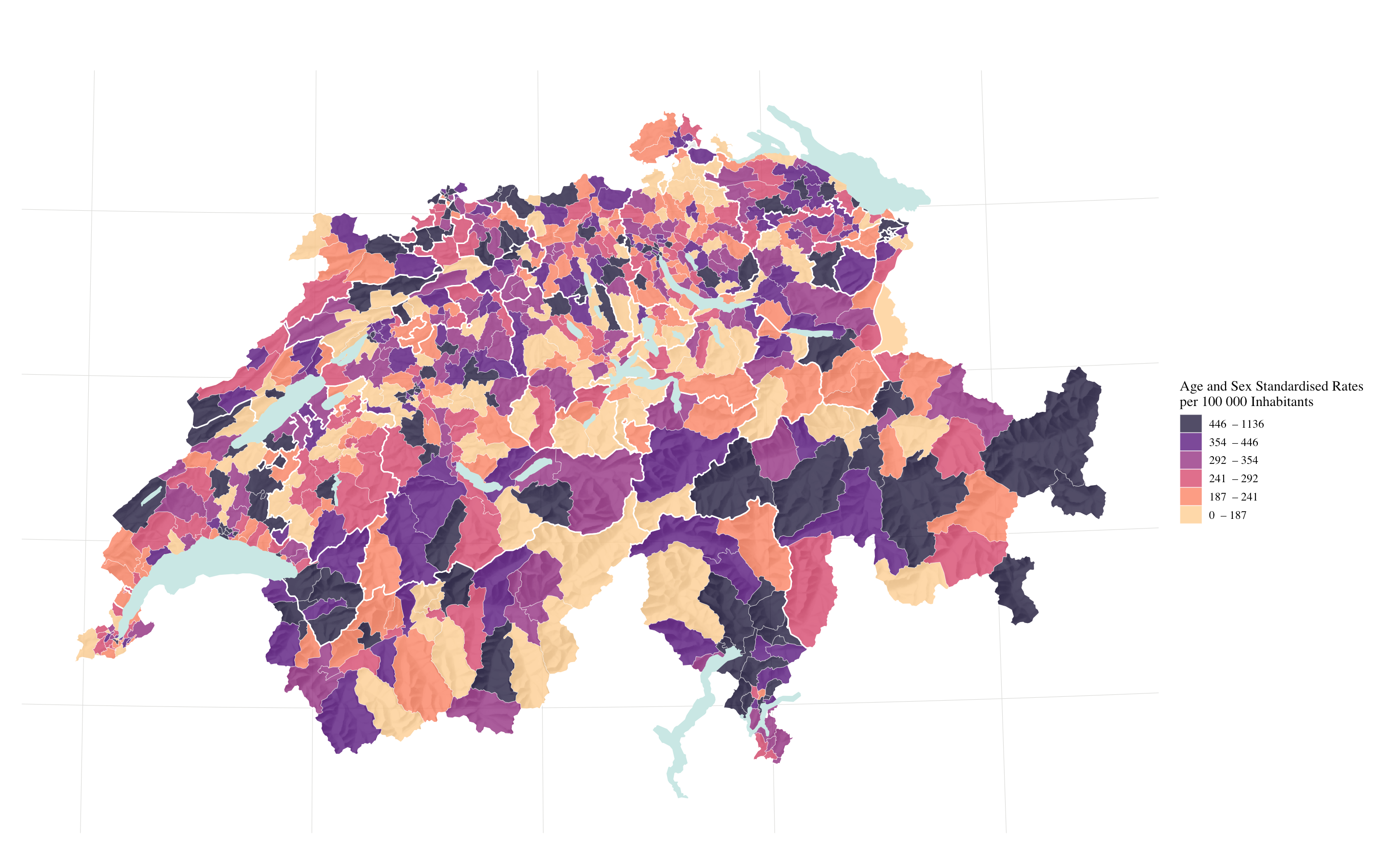
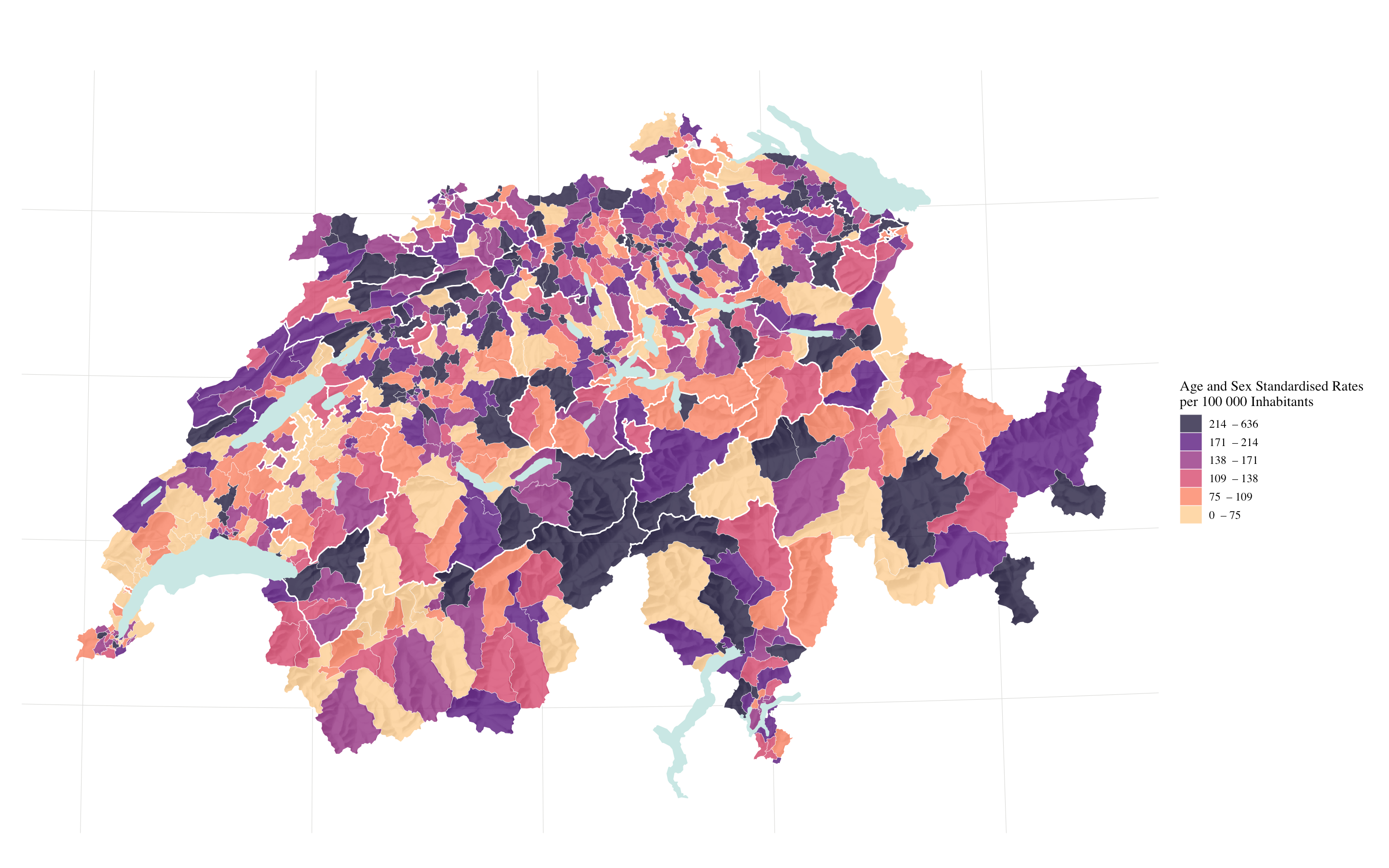
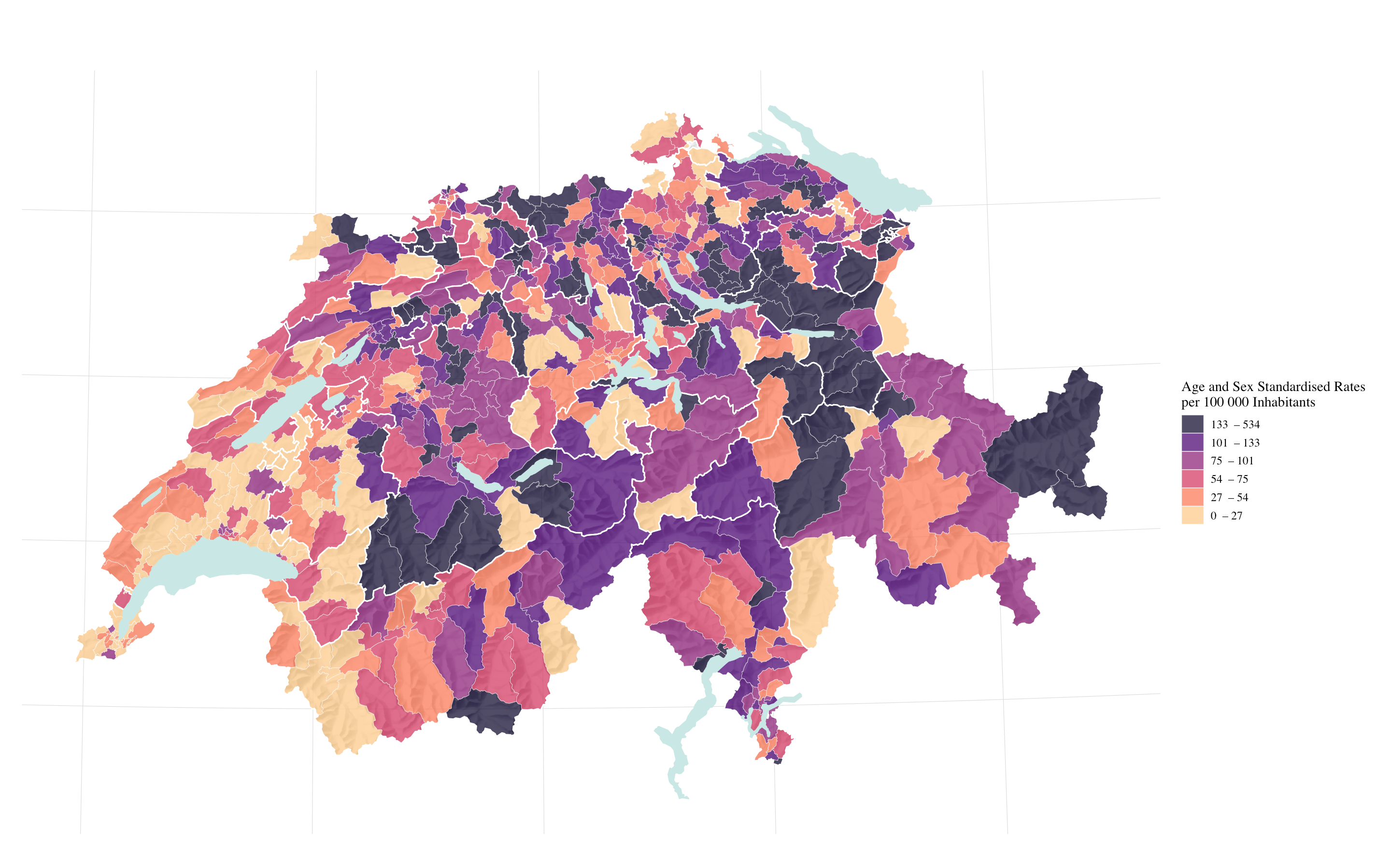
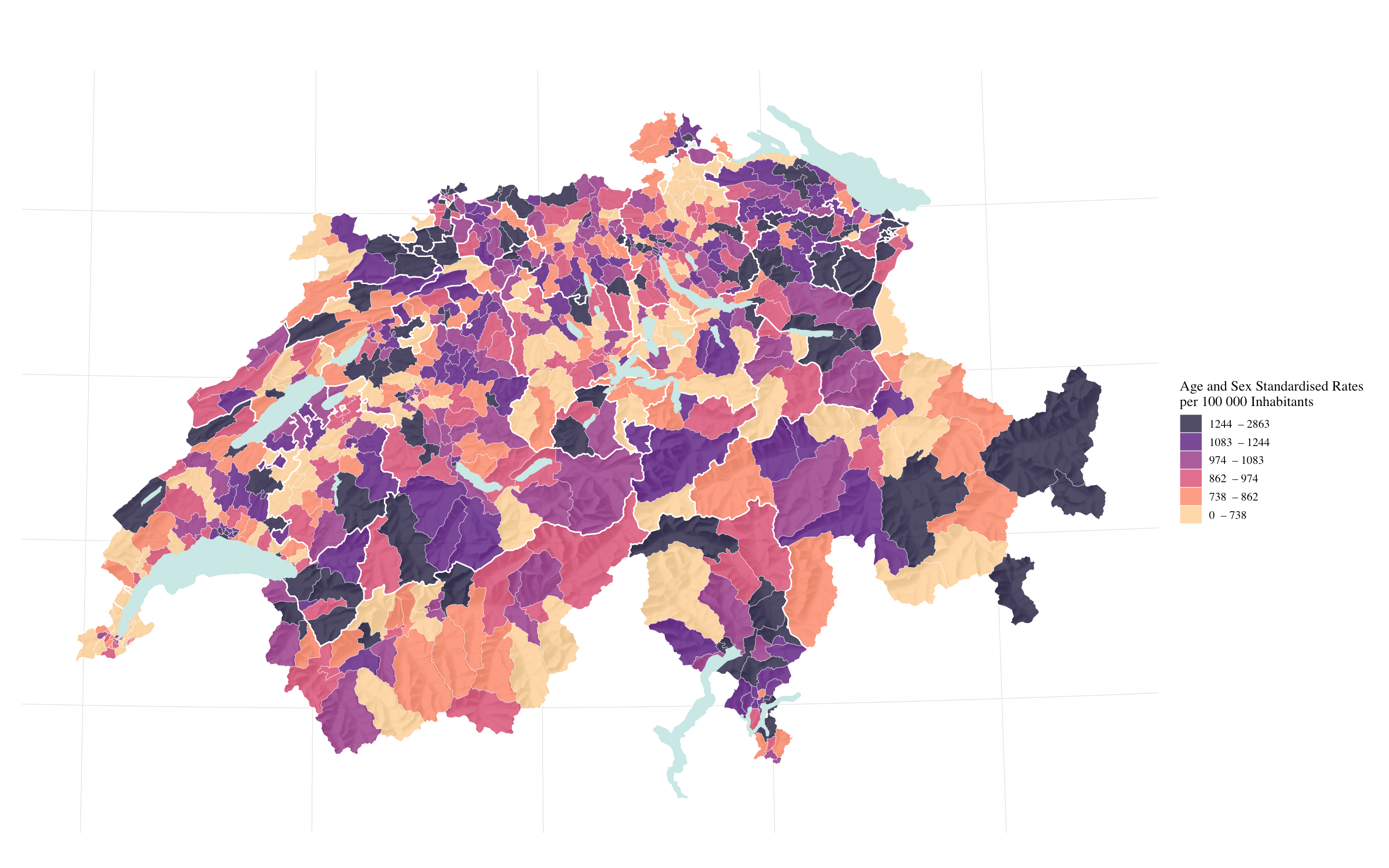
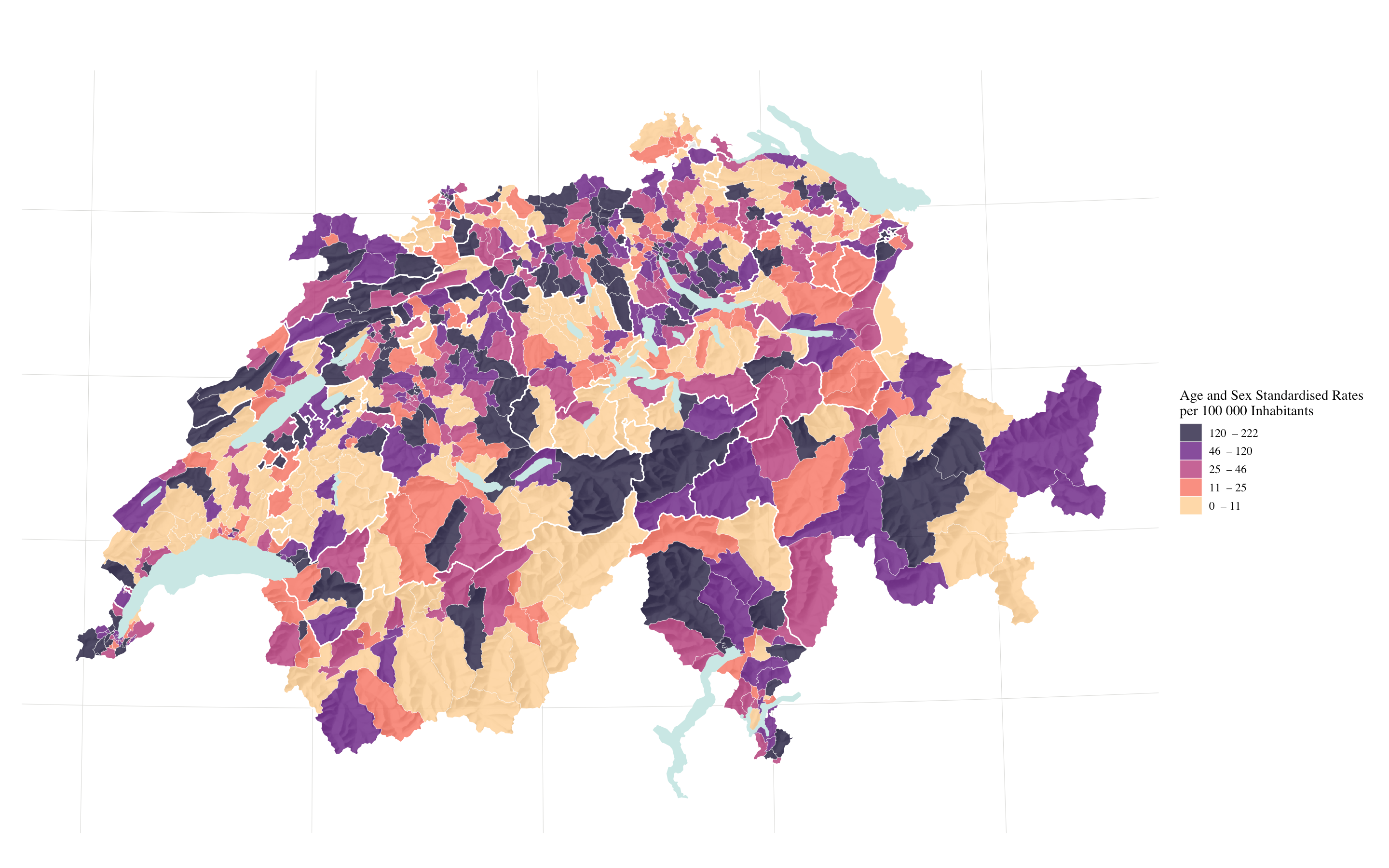
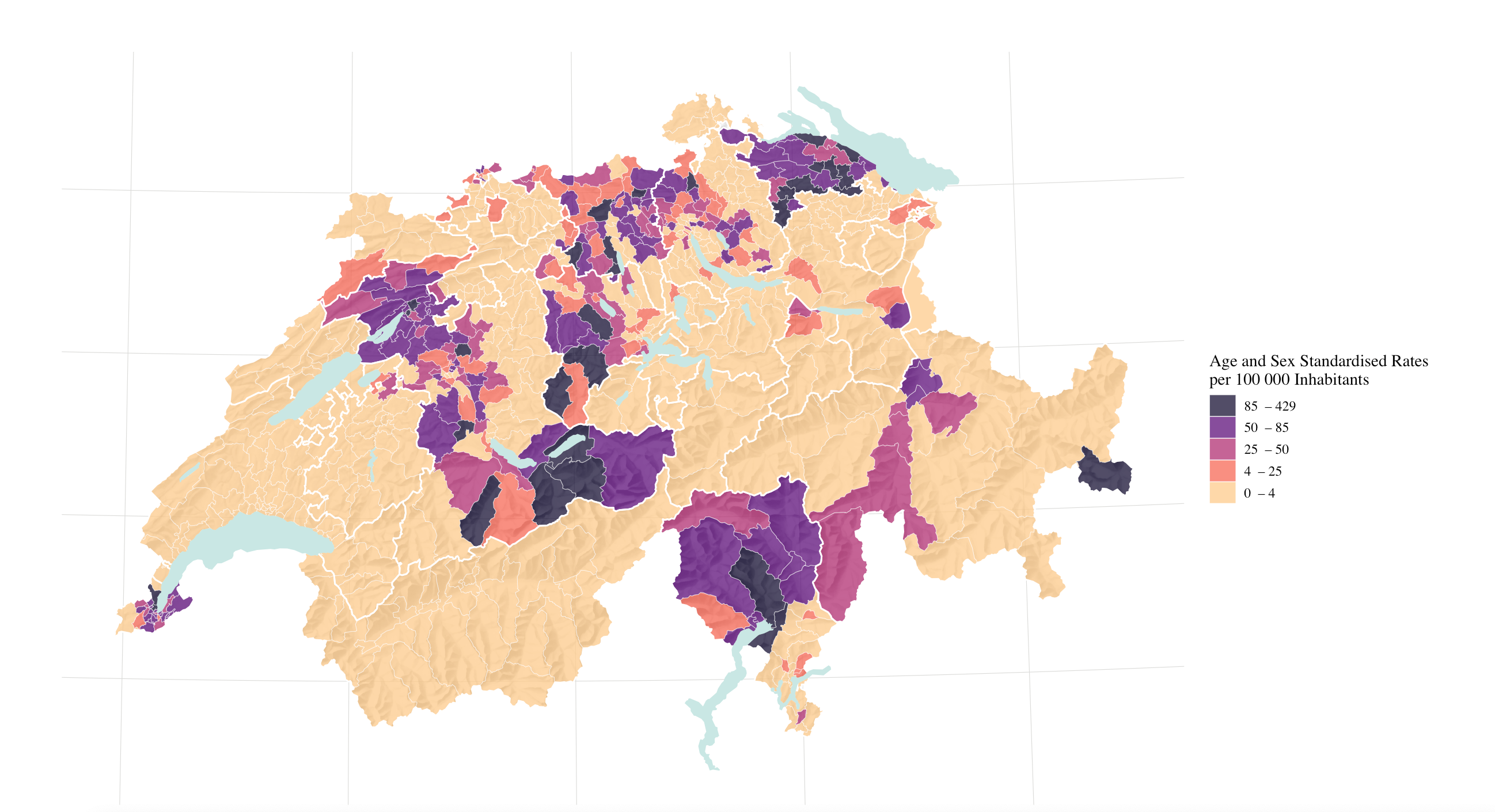
The findings suggest a high degree of variation amongst HSA and cantons regarding avoidable hospitalisations for all ACSCs. Moreover, we found pronounced geographical patterns based on both diagnosis and setting. Most prominently, variation in the management of angina pectoris shows substantial variation in Switzerland’s northern and north-eastern regions. Interestingly, when assessing rates of congestive heart failure, these patterns shift towards the southwest. Regarding hypertension, though, we found consistently lower rates in the southwest. While these patterns indicate some of the challenges HSAs and cantons face in providing specialized primary health care for different diseases, they also underscore the importance of differentiating between diseases and visualizing results to address issues in primary health care provision.
The broad regional variation for the various diagnoses may reflect specific regional (cantonal) approaches to primary care provision. Evidence supports the possibility that socioeconomic, demographic and provider specific determinants contribute to the emergence of avoidable hospitalisations for ACSCs (13, 17, 37-40). Switzerland’s primary health care system is stable and functional, and its income inequality quite low (2, 16-19). Rather than access to affordable medical advice, contributing factors might include regional differences in compensation structures for both primary and hospital care, as well as the proximity and density of hospitals, primary health care networks and regional public health programs. While it remains unclear just how these factors affect the rates of ACSC-related hospitalisation, minimizing those rates will demand an understanding of the contributing factors.
Contributing Factors and Impulse for Health Policy
Evidence suggests that physician density, healthcare accessibility, resources for primary health care and continuity of care are all related to rates of avoidable hospitalisation for ACSCs (2, 41-45). In Switzerland, except in some isolated alpine regions, accessibility to primary health care is consistently high (46), i.e., resources for primary health care were reinforced in 2014, and physician density is sufficient. More physicians might actually lower healthcare efficiency: several studies suggest that high physician density can inflate demand for health care services (2, 40, 47).
The issue of regional variation and the high rates of avoidable hospitalisation for ACSCs despite high accessibility to and adequate resourcing for primary care might be an indication that continuity of care plays a crucial role. Continuity of care should focus on a team-based approach to reduce fragmentation of care and improve patient safety and quality of care (48). Focussing of chronic care management might provide useful guidance to improve continuity of care. Chronic care management in Switzerland is still predominately provided by primary care physicians. With Switzerland’s primary care physician workforce aging this may eventually lead to a shortage of general practitioners and disrupt chronic care management (16). Chronic care management for specific populations might therefore require novel roles in care delivery for the chronically ill (49). Interventions to reduce hospitalisations for ACSC include specialized home care, promotion of self-management and the integration of primary and secondary care (50). Complementary to established primary care models nurse-led models can be part of such interventions. Advanced practice nurses already play crucial roles in specialized and primary care delivery, improving outcomes in chronic care management, e.g., reduced hospitalisations or improved blood pressure management, as compared to established models of care (51, 52). Advanced practice roles such as nurse practitioners can perform many tasks of chronic care management such as promoting self-management and care coordination. However, such roles are currently underdeveloped in Switzerland and limited to a small number of collaborative efforts (53, 54). Hence, nurses can only provide limited resources in Switzerland. Collaboration with different primary care providers such as physiotherapists, dietitians, occupational therapists is crucial to address self-management and ultimately reduce hospitalisations for ACSC. Swiss health policy makers could address these challenges by promoting these approaches to bridge the gap in chronic care management and to improve continuity of care.
The geographical representation and small area approach differentiated by diagnosis and care structure highlight the various Swiss regions’ relative success at minimizing avoidable hospitalisations. There is a need to understand the specific context and its impact on continuity of care. Health policy makers should address these regional variations with a distinct focus on strengthening continuity of care for the chronically ill.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}