To the best of our knowledge, this study is the first to investigate clinical outcomes following treatment of bifurcation lesions using two different 2-stent techniques, DK culotte versus culotte, in a real-life ACS cohort.
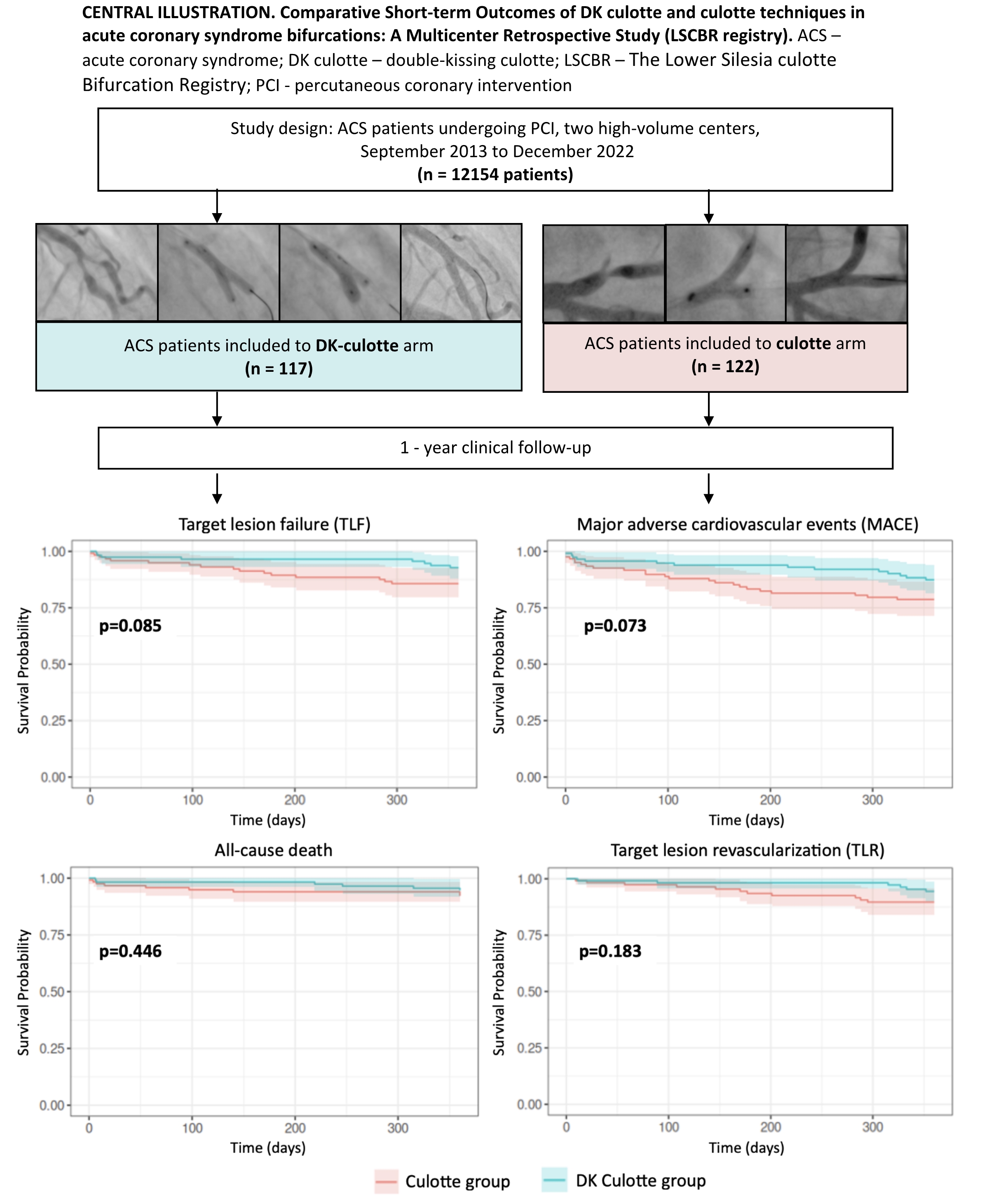
The study results did not show a statistically significant difference between the two stent techniques in terms of 1-year follow-up. However, there was a trend towards a lower incidence of 1-year TLF and MACE in the DK culotte group compared to the classic culotte group, primarily due to a lower number of TLR events. Statistical significance could have been achieved with a longer follow-up period or larger study groups. Additionally, no significant differences in contrast volume or radiation dose were found between the two evaluated stenting techniques. The DK culotte technique facilitated achieving a 100% success rate in the final-KB procedure.
According to the revascularization guidelines[15], provisional stenting is the most applicable solution in most bifurcation cases. However, operators may need to consider a two-stent technique in more complex coronary bifurcation anatomies, especially in the ACS subset where preserving good flow to the SB may be crucial to achieve a favorable clinical outcome and potentially reduce ischemic burden. Several anatomical features may encourage this approach. Procedural factors that influence the adoption of up-front two-stent strategies include a large SB (≥ 2.75 mm) with a long ostial lesion (at least > 5 mm), anticipated difficulty in accessing the SB after MB stenting, and true bifurcation lesions [16, 17]. Recently published data indicate that a systematic two-stent approach may be associated with a significant improvement in clinical outcomes compared with classical single-stent technique in patients with complex bifurcation lesions[18].
The bifurcation consensus document[3] by the European Bifurcation Club listed three main two-stent techniques: “T/TAP”, “culotte”, and “DK-crush”. Since the development of DK-crush by Chen et al.[19], several landmark trials have demonstrated the safety and efficacy of this technique, particularly compared with classic crush. A modification to the classic crush technique, involving the addition of an extra KB inflation, has significantly improved the long-term results of the DK crush. Various studies revealed that KB inflation is a crucial aspect of bifurcation management.
Since its introduction to clinical practice[7], the technically demanding bifurcation stenting technique known as Culotte, has become widely used because of its satisfactory safety and efficiency[8,20]. However, some data indicate that the DK-culotte technique may provide benefits over culotte[21, 22]. Recent bench testing reveals that performing additional KB dilatation before stenting the second branch may improve the culotte technique[10]. This reduces the risk of pulling the struts of the first stent toward the ostium, which could affect the procedure's progress and the ability to perform a final KB inflation. The latter is crucial for achieving optimal results.
Therefore, this simple modification is a new cornerstone for improving the culotte technique. However, clinical studies that investigate the significant effects of adding KB to culotte technique, on long-term outcomes remain lacking. The results of this multicentre retrospective analysis are the first available data on the short-term prognosis of the DK Culotte method compared to the Culotte method. Additional KB step is a safe method for modifying the Culotte technique facilitating the performance of the final KB procedure. Further follow-up is recommended to determine any distant benefits.
{kind=link}