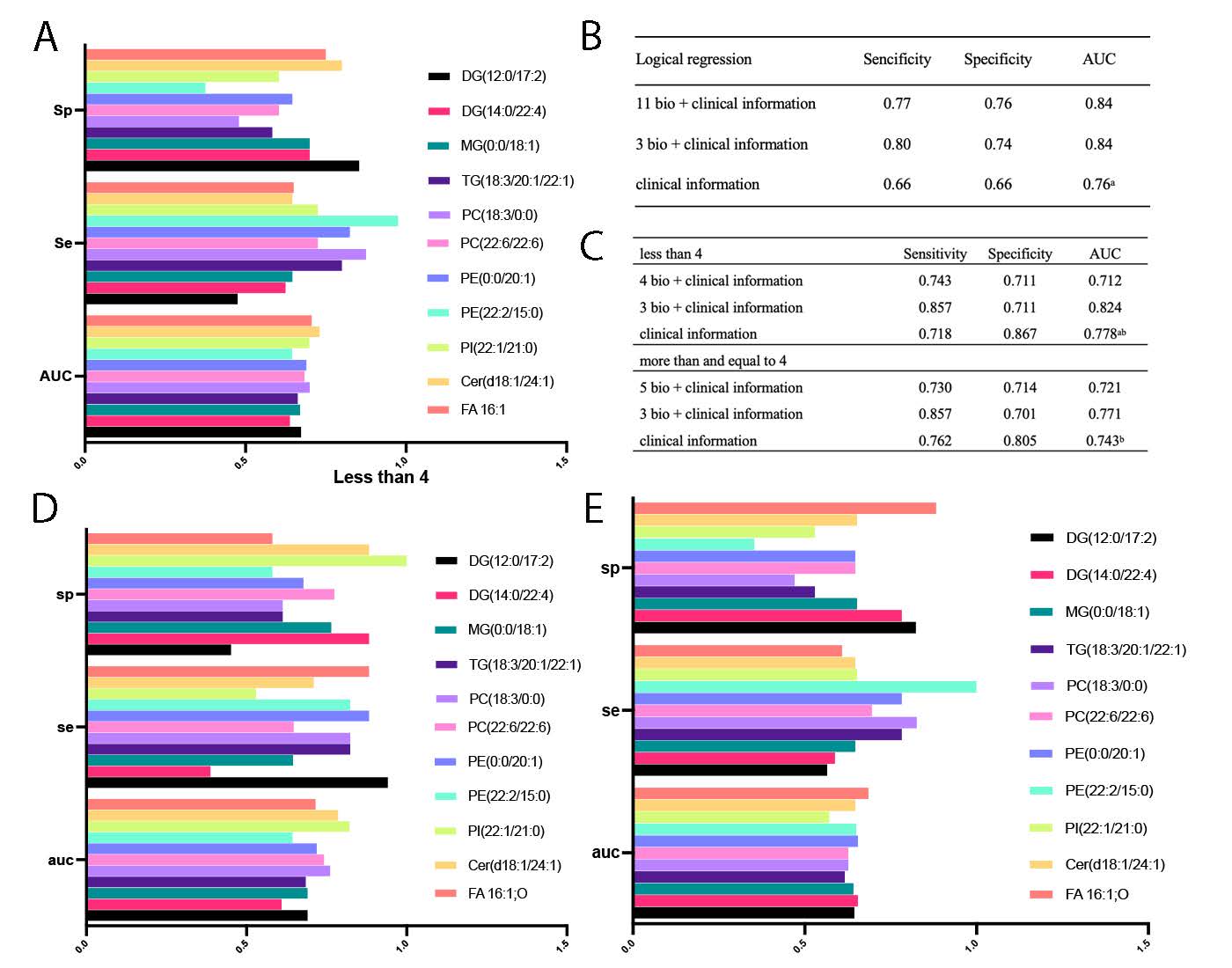
This study employed a UPLC-MS/MS platform for lipidomic analysis to identify features associated with the occurrence of stroke in patients with LA. Previous investigations have indicated that severe leukoaraiosis (sLA) could serve as a significant adverse factor affecting early neurological recovery following mechanical thrombectomy (MT), potentially diminishing favorable outcomes in acute ischemic stroke (AIS) patients undergoing MT[28–30]. The recent BEST trial demonstrated that moderate to severe leukoaraiosis (LA) was linked to poorer outcomes among patients receiving endovascular treatment[31]. Significant alterations in lipids between LA and LS included glycerolipids, glycerophospholipids, sphingolipids, and fatty acids (Fig. 3A). Through structural equation modeling and pathway analysis, we selected 11 key metabolites that exhibited excellent performance in distinguishing between LS and LA (AUC = 0.840) (Fig. S1B). Additionally, these key metabolites also demonstrated efficacy within subgroups (Table S6 and Fig. S1C-D).
White matter damage in the brain is often linked to the aging process and chronic conditions such as hypertension, as well as various diseases[32]. The impact of white matter lesions becomes particularly significant in patients diagnosed with LA, who faced an elevated risk of stroke[33]. Kongbunkiat et al. conducted a meta-analysis involving 15 studies with a total of 5,967 participants[34]. They reported a relative risk (RR) of 1.65 (95% confidence interval [CI] 1.26–2.16, p = 0.001) for the occurrence of symptomatic intracerebral hemorrhage (SICH) in patients with LA, translating to an absolute risk (AR) increase of 2.5% compared to those without LA[34]. This consistent association indicates that the presence and severity of LA are linked to a heightened risk of SICH following thrombolysis for acute ischemic stroke (AIS). The elevated risk of intracerebral hemorrhage (ICH) post-thrombolysis in acute cerebral infarction patients with LA may be attributed to factors such as vascular endothelial injury, increased platelet activation, and hypercoagulability[34]. Additionally, in individuals undergoing anticoagulant treatment, the presence of LA was correlated with an augmented likelihood of recurrent stroke and intracranial hemorrhage[35]. Nevertheless, conventional risk factors exhibit limitations in fully predicting LA in patients who have experienced a stroke. Lipidomics, an analytical approach focusing on the detection of lipid metabolites at the systemic level, holds promise in uncovering potential biomarkers, identifying lipid metabolic pathways, and constructing networks of lipid metabolism[36]. A systematic review comprehensively outlined potential metabolic biomarkers and pathways associated with ischemic stroke, underscoring the consistent identification of several metabolites with biomarker potential[37]. Additionally, metabolomics analysis using machine learning techniques was performed on plasma samples from ischemic stroke patients and controls, revealing three key differential lipid metabolites[38]. Furthermore, our previous research has identified lipid biomarkers associated with cardioembolic and atherosclerotic stroke[26].
Pathway analysis indicated that glycerophospholipid metabolism actively participate in both LA and LS groups (Fig. 2H). Concurrently, we observed a significant decrease in glycerophospholipids in the LS group (Fig. 3). Glycerophospholipids are an important part of the neuronal cell membrane structure and are involved in cell recognition and signal transduction. Therefore, the degradation of glycerophospholipids, which produces polyunsaturated fatty acids such as docosahexaenoicacid and arachidonic acid, may be a sign of brain damage[39, 40]. A previous study has indicated that glycerophospholipid metabolism was significantly disrupted in stroke rats. These findings suggest that the decreased levels of glycerophospholipids in the hippocampus may play a role in the pathophysiology of stroke[41]. Our study confirmed that during the progression of cerebral white matter stroke, glycerophospholipid metabolism was abnormally inhibited (Fig. 3).
Through pathway analysis and SCE model, we selected 11 key metabolites between LA and LS groups. There were DG(12:0/17:2), DG(14:0/22:4), MG(0:0/18:1), TG(18:3/20:1/22:1), PC(18:3/0:0), PC(22:6/22:6), PE(0:0/20:1), PE(22:2/15:0), PI(22:1/21:0), Cer(d18:1/24:1), FA16:1 O (Fig. 4). We identified these key metabolites to be concentrated in monoglyceride, diglyceride, triglyceride, phosphatidylinositol, phosphatidylethanolamine, phosphatidylcholine, ceramide, and fatty acids. The primary role of triglycerides is for the storage and provision of energy[42]. Triglycerides consist of saturated fatty acids (SFAs), monounsaturated fatty acids (MFAs), and polyunsaturated fatty acids (PFAs)[43]. The decreased of TG(18:3/20:1/22:1) observed in LS compared to LA may be associated with an activated inflammatory response (Fig. 4D)[44]. Our findings suggest that the perturbed equilibrium in triglyceride metabolism could be linked to an inflammatory response. The demyelinating effects of LA impair the network connectivity within the brain to differing extents, influencing specific neurotransmitter conduction pathways in the white matter (WM)[45]. The preservation of normal cognitive functions is intricately tied to the integrity of the cholinergic pathway in the brain, which forms intricate connections with regions such as the prefrontal cortex, ventral striatum, and hippocampus/amygdala[45]. Our investigation results also indicated a noteworthy association between the dysregulation of diglyceride, lysophosphatidylcholine (LPC), and phosphatidylcholine, and an increased susceptibility to stroke (Fig. 4. C and J-K). We also found that higher levels of Cer(d18:2/24:1) were associated with LS (Fig. E4). Neuroinflammatory processes, characteristic of demyelinating diseases like multiple sclerosis (MS), contribute to myelin sheath damage[46]. Previous investigations have demonstrated heightened cerebrospinal fluid (CSF) concentrations of sphingomyelins and ceramides in individuals with multiple sclerosis and other demyelinating conditions[47, 48]. Based on biological significance, we conducted multivariable regression analysis and identified DG(14:0/22:4) (OR = 5.33, p = 0.02) and Cer(d18:1/24:1) (OR = 21.44, p = 0.068) as risk factors for stroke with LA. Concurrently, linear regression analysis revealed a significant negative correlation between FA16:1, O, DG(12:0/17:2), and DG(14:0/22:4) and Fazekas scores (Fig. 5C-F). We also conducted a 7-fold cross-validation, revealing strong predictive performance for these combinations (Fig. S1A-B). We ultimately confirmed the involvement of glycerolipid metabolism, glycerophospholipid metabolism, and sphingolipid metabolism in the pathway of associated with stroke in patients with LA (Fig. 7).
Potential mechanisms by which LA exacerbates the impact of ischemic stroke encompass hypoxia, vascular endothelial injury, disruption of the blood-brain barrier, and impairment of brain connectivity[4]. Hypoxia-ischemia is believed to contribute to the etiology of neurotrophic acid (LA)[49, 50]. Brain hypoxia primarily arises from small vessel disease, particularly affecting arteries like the thalamostriate and other perforating arteries[51, 52]. Neuropathological investigations have revealed that LA, as observed on CT or MRI scans, correlates with demyelination, astrocytic gliosis, arteriolosclerosis, dilated perivascular spaces, and frequently coexists with lacunar infarcts[53]. Our previous research found that phosphatidylcholine (PC) significantly decreases under hypoxic conditions[54], which is consistent with the results of this study(Fig. 7).
Some studies discovered significant blood-brain barrier leakage in the normal white matter of stroke patients, which became more severe the closer they were to white matter hyperintensity (WMHs), while blood-brain barrier dysfunction increased with increasing WMH load[55–57]. Based on the Fazekas score, patients in the LA and LS groups were divided into two subgroups (Table S4). Through logistic regression model analysis, a specific combination (PC(18:3/0:0), Cer(d18:1/24:1), FA 16:1;O, and clinical information) was found to have high predictive value for adverse cardiovascular events under conditions of lower Fazekas scores(Fig. S1C-D). Some studies have confirmed the significant role of plasma Cer(24:1) concentration in predicting referrals for coronary angiography in different populations[58–61]. These results indicated a notable association between elevated plasma sphingolipid concentrations and adverse cardiovascular events[59–61]. Harshfield's investigation had revealed a positive correlation between higher levels of SM(d18:2/24:1) and measures such as fissure count, WMH volume, and cognitive abilities[62]. Our study further substantiated a significant elevation in Cer(d18:1/24:1) within the LS group, regardless of whether the Fazekas score is less than 4 or more than or equal to 4.
LA and patients with acute cerebral infarction share common risk factors, including advanced age, hypertension, diabetes, smoking, and alcohol consumption[4]. With the exception of age, which cannot be controlled, targeting the aforementioned risk factors is of paramount importance for both primary and secondary prevention strategies. Our study, through an in-depth exploration of metabolic biological processes, provides a theoretical basis and assistance for the future prevention and treatment from LA to LS. However, this study has some limitations. The current validation is limited to self-validation, and further studies are needed to validate and optimize the discovered biomarkers and evaluate their effectiveness in terms of clinical application. Therefore, in future studies, we should select purer samples and expand the sample size to further investigate the biomarkers of these findings and evaluate their clinical applicability in screening and diagnosing stroke in individuals and patients with LA. This will contribute to the improvement of screening and diagnostic methods for individuals with LA and stroke in patients with LA, enabling clinicians to develop more personalized treatment strategies.
{kind=link}