2.1. Overview.
In the present experiments, we examined the antinociceptive effects of both systemic and spinal administration of baclofen. We used several models of bladder nociception with endpoints which included spinal dorsal horn neuronal responses, UBD-evoked changes in arterial blood pressure and the VMR (abdominal contractions) evoked by UBD. In addition to normal, healthy rats, we also assessed responses in rats whose bladders were made hypersensitive to bladder distension by inflammation. These studies were all approved by the UAB Institutional Animal Care and Utilization Committee.
2.2 Animal Subjects.
A total of 205 Sprague-Dawley female rats obtained from Harlan/Envigo (Prattville, AL) were used as adults (mean weight 283 ± 12 gms) in all experiments. In some experiments, rats were raised from birth, treated as pups and allowed to mature to adulthood (description in Sect. 2.4). All rats were housed with food and water available on an ad libitum basis. A 12:12-h light:dark cycle was maintained, where lights were off between 6:00 pm and 6:00 am. There was no attempt to control for estrous cycle, as the focus of this study was not on estrous-related changes in pain, and we have previously shown that hormone fluctuations due to the estrous cycle do not alter the vigor of UBD-evoked VMRs in rats without bladder inflammation when the current methodology is employed34.
2.3. Adult Bladder Inflammation (ABI).
As adults, some rats received a treatment 24 h prior to UBD testing on the following day. At that time, animals were anesthetized with inhaled isoflurane and oxygen (5% for induction, 2% for maintenance) and separated into groups receiving either no treatment or intravesical zymosan. Intravesical zymosan treatment has been demonstrated to produce a robust bladder inflammation and hypersensitivity to UBD35. Zymosan-treated animals had their urinary bladders catheterized with a 22-gauge angiocatheter via the urethra. Zymosan (0.5 ml, 1% in saline) was administered intravesically for 30 min and drained. Rats in the anesthesia only control group were maintained on 2% isoflurane for 30 minutes, immediately after induction with 5% isoflurane. All animals received ampicillin at the end of the procedure (50–100 mg/kg, s.c.).
2.4. Neonatal Bladder Inflammation (NBI).
Some groups of female rat pups were given three daily neonatal treatments of zymosan beginning on post-natal day 14 (P14-16). Each rat was anesthetized with isoflurane (5% induction; 2% maintenance) delivered by mask. In one group, a 1% zymosan (0.1ml) solution was instilled intravesically via a 24 gauge angiocatheter placed through the urethra and allowed to dwell for 30 min. The bladder then was drained, the catheter removed, and the rat permitted to recover. The control group only received anesthesia and no catheterization or zymosan treatment. All rats were kept on a warmed heating pad during treatments and received ampicillin (0.05 mg in 0.05 ml s.c.) at the end of each treatment before being returned to their dams. All rats were weaned at 3 weeks and then raised to adulthood before use (12–15 weeks of age). This treatment has been demonstrated to produce hypersensitivity to UBD and is described more completely elsewhere36.
2.5. Reflex Responses to Urinary Bladder Distension (UBD).
Animals were anesthetized with urethane (1.2 g/kg s.c.) and/or isoflurane (2–5% during surgery, later reduced to < 0.75%). A 22-gauge polytetrafluoroethylene angiocatheter (Johnson and Johnson, Arlington TX) was placed into the bladder via the urethra and held in place by a tight suture around the distal urethral orifice. Silver wire electrodes were inserted into the external oblique musculature immediately superior to the inguinal ligament for recording of abdominal EMG activity. In some cases, a carotid arterial catheter was placed to allow for hemodynamic measures. Following surgery, anesthesia was reduced until flexion reflexes were present in the hind limbs but spontaneous escape behaviors were absent. In most experiments, the primary response measure was the visceromotor reflex (VMR), an abdominal contraction evoked by UBD which consisted of air distension of the urinary bladder using the intravesical catheter. An in-line, pneumatically-linked, low volume pressure transducer was used to monitor intravesical pressure. VMRs, recorded as electromyographic activity of the abdominal musculature, was measured via the electrodes using standard differential amplification and rectification and saved on a computer (Spike 2 software, Cambridge Electronic Design, UK). “Evoked” VMR responses were defined as the mean rectified electromyographic activity (in mV) during 20 s of UBD minus the mean baseline electromyographic activity (in mV) measured in the period immediately preceding the onset of UBD. Hemodynamic responses to UBD were defined as the maximal sustained change in mean arterial pressure measured during UBD minus the mean arterial pressure measured immediately prior to UBD. This model system has been described more extensively elsewhere37,38.
2.6 Intrathecal Catheters.
In experiments in which selective spinal action of drugs was studied a 7.8 cm catheter made of PE10 tubing was inserted via an incision in the atlanto-occipital membrane following surgical exposure and threaded down through the subarachnoid space to the lumbosacral region under deep isoflurane/oxygen anesthesia. In most cases, the catheter was used immediately in non-survival experiments (as per Sect. 2.8), but in 13 rats the catheter was attached to an Alzet 2001 osmotic minipump (Durect Corp, Cupertino, CA, USA) allowing for a 7-day infusion of either normal saline or a baclofen solution as described in Sect. 2.11.
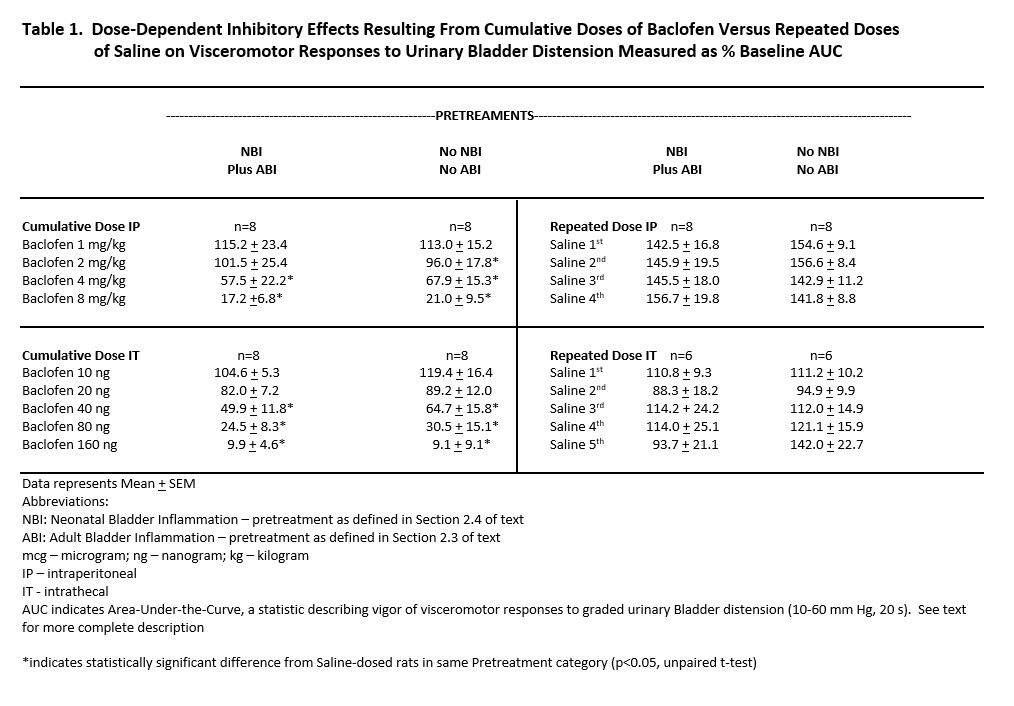
2.7 Protocol for Systemic Baclofen Cumulative Dosing Experiments.
Repeated 60 mmHg UBDs were administered with a 3 min inter-trial interval until stable VMRs were established. Graded, constant-pressure air distensions of the urinary bladder (20 sec duration; 3 min inter-trial interval) of ascending pressures at intervals of 10, 20, 30, 40, 50 and 60 mmHg were then administered to quantify the graded stimulus-response. A cumulative dosing paradigm was then initiated with consecutive doses of 1, 1, 2 and 4 mg/kg of baclofen (Sigma-Aldrich, St. Louis, MO, USA; Cat. No. B5399) or equal volumes of normal saline (1 ml/kg) administered IP for cumulative doses of 1, 2, 4 and 8 mg/kg respectively in the case of baclofen. The saline injections served as a repeated measures control procedure. Fifteen minutes following each injection graded stimulus-response measures (10–60 mm Hg, 20 s UBDs) were re-determined using the method described above.
2.8 Protocol for Spinal Baclofen Cumulative Dosing Experiments.
Rats were prepared following a surgical procedure similar to that used in Sect. 2.6, but with the addition of an acutely placed IT catheter. A protocol similar to that described in Sect. 2.6 was then performed using consecutive doses of 10, 10, 20, 40 and 80 ng of baclofen (or equal volumes of normal saline) dissolved in 10 µl of normal saline followed by a 10 µl normal saline flush through the IT catheter. Graded stimulus-response measures were determined 15 minutes following each baclofen/saline injection.
2.9 Protocol for Assessing Effects on Hemodynamic Responses to UBD.
In these rats, a single 40 ng dose of IT baclofen (10 µl injection; 10 µl normal saline flush) or equal volume of IT normal saline was administered and responses to repeated UBDs (60 mm Hg, 20 s, 3 min intervals) measures, allowing for assessment of the time course of the baclofen effect. In this case, responses included both VMRs and hemodynamic responses measured using a carotid arterial catheter. The IT saline-treated rats served as a control for repeated measures.
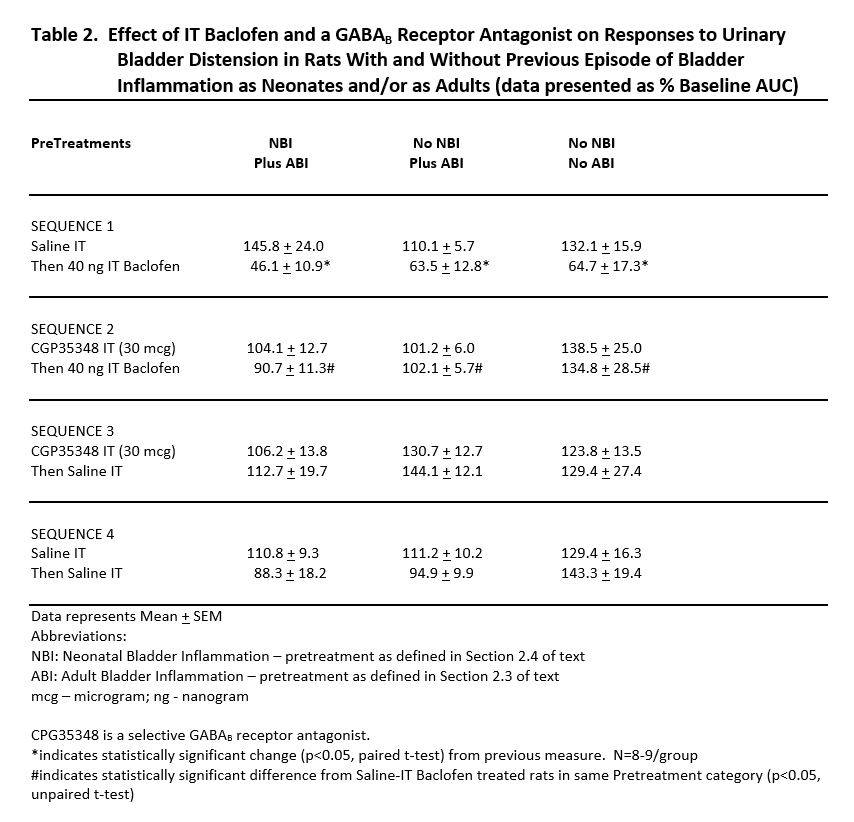
2.10 Protocol for Assessing Actions of Baclofen Via GABA-B receptors.
To verify that baclofen was acting through GABAB receptor mechanisms, an antagonist was administered IT prior to administration of baclofen. Specifically, these rats received repeated UBDs (60 mm Hg, 20 s 3 min ITI). After VMRs to UBD were stable (+/- 20%), responses to graded UBD (10–60 mm Hg, 20 s) were obtained. Rats then received a single IT injection of either CGP35348 (30 µg; Tocris Biosciences, Minneapolis, MN, USA; Cat. No. 1245) or an equal volume of normal saline (10 µl) followed by a 10 µl normal saline flush. Fifteen minutes after the injection repeat graded UBD stimulus-response measures were obtained. Rats then received an IT injection of baclofen (40 ng) in normal saline or an equal volume of normal saline (10 µl) followed by a 10 µl normal saline flush. Fifteen minutes after this injection, repeat graded UBD stimulus-response measures were obtained. These dosing combinations resulted in three separate measures in four separate groups.
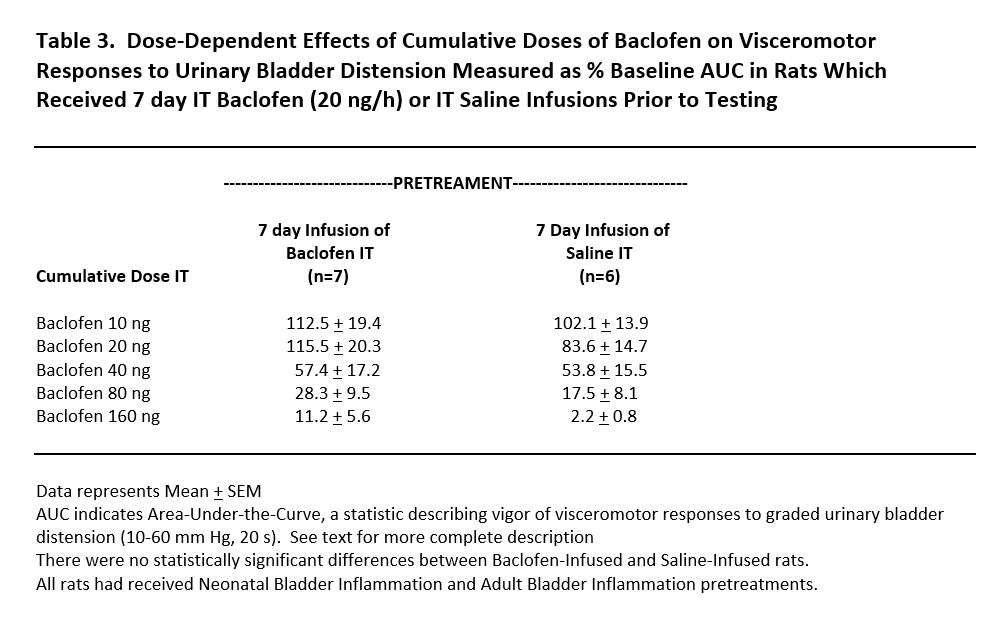
2.11 Protocol for Assessing Tolerance to Spinal Baclofen.
Thirteen rats which had received neonatal bladder inflammation (Sect. 2.4) had IT catheters placed (Sect. 2.5) and attached to seven day minipumps that were then secured in the subcutaneous tissues between the rats’ scapulae. Incisions were closed with sutures and the rats allowed to recover. Half of the rats received an infusion of baclofen at a rate of 1 µl/hr or 20 ng/hr for 7 days. The other half of the rats received a normal saline infusion at the same rate. The day before testing, all rats were re-anesthetized with isoflurane, adult bladder inflammation induced (Sect. 2.3) and their IT catheters externalized and minipumps removed. They were allowed to recover overnight and then underwent cumulative dosing of IT baclofen in a fashion identical to that noted in Sect. 2.8.
2.12 Dorsal Horn Spinal Neuronal Responses to UBD.
Animals were anesthetized with isoflurane (5%) and a tracheal cannula placed allowing for mechanical ventilation. The cervical spinal cord was exposed surgically, injected with 50 µl of 1% lidocaine solution and subsequently transected using a sharp scalpel. The brain was then pithed mechanically, anesthesia discontinued and the rats allowed to recover until demonstrating robust hindlimb flexion reflexes in response to paw pinching (typically 1–2 hours). A laminectomy was then performed and the dura incised exposing the L6-S2 spinal segments since these are known sites for spinal processing of afferent information from the bladder. The vertebral column was clamped both rostrally and caudally to the laminectomy for stabilization. Skin flaps were arranged to form a protective coating for exposed tissue except for the site of recording which was covered with warmed mineral oil. A PE10 catheter was secured at the edge of the exposed spinal dorsal horn for future use in the topical administration of drugs. Tungsten microelectrodes (MicroProbe, Clarksburg, MD; 1.2–1.8 MOhm) were used for conventional extracellular single-unit recording. The dorsal horn 0–1.0 mm from midline and 0-1.2 mm below cord dorsum was searched using microelectrodes positioned using a stereotaxic apparatus. All units responded in a consistent excitatory fashion to UBD. To quantify neuronal responses, units were displayed oscillographically for continuous monitoring, discriminated conventionally from background, converted into uniform pulses and counted and saved by computer. The total number of unit action potentials (discharges) were counted in 10 s epochs before, during and after the UBD stimulus. Evoked Activity of the dorsal horn neurons was defined as the number of unit discharges during UBD minus the level of activity immediately preceding the onset of UBD. Because responses of different neurons to the same distending stimulus naturally vary in maximal response and total number of unit discharges, each unit’s response was normalized to that produced by the 60 mm Hg response for purposes of within- and between-group comparisons. Noxious and non-noxious somatic stimuli were also presented to each neuron and excitatory/inhibitory responses determined in a fashion similar to that which we have previously published39. Following characterization, the effect of the spinal application of 160 ng baclofen or an equal volume of normal saline (20 µl) on spinal dorsal horn neuronal responses to repeated UBD (60 mm Hg, 20 s; 3 min intervals) was determined by measuring multiple responses prior to and following drug administration. All of the rats studied in this protocol had also experienced neonatal bladder inflammation and adult bladder inflammation as per Sect. 2.3 and 2.4.
2.13 Statistical Analyses.
Statistics are presented as the mean ± S.E.M in the graphs. Area-Under-the-Curve (AUC) statistics were generated as measures of global responses to graded UBD and reported as a percentage of mean pre-drug measures. In some studies, repeated measures ANOVAs were performed followed by post-hoc analyses of means when appropriate. Paired t-tests of pre/post measures were used for comparisons when appropriate.
{kind=link}
{kind=link}
{kind=link}