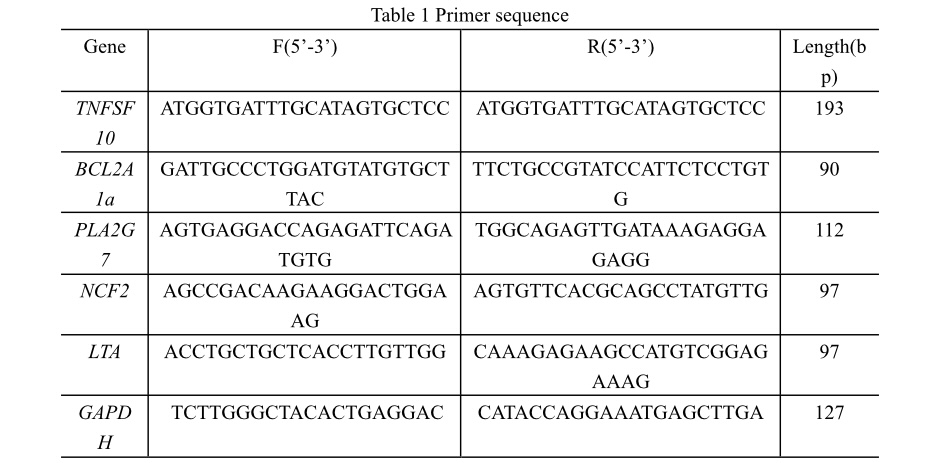
Polycystic Ovary Syndrome (PCOS) is recognized as a multifaceted endocrine-metabolic disorder, with current diagnostic protocols largely adhering to the Rotterdam criteria established in 2003[6]. These criteria encompass hyperandrogenemia, infrequent ovulation or anovulation, and polycystic ovarian morphology, requiring the presence of any two for a PCOS diagnosis. Despite these criteria, PCOS diagnosis often experiences delays, typically involving consultations with multiple physicians over a period extending beyond two years[7]. The urgency to refine PCOS diagnostic and treatment paradigms is underscored by the escalating adverse outcomes associated with the syndrome. Recent insights highlight mitochondrial oxidative stress and chronic inflammation as primary etiological factors, linked to hyperglycemia, anovulation, hyperandrogenemia, and insulin resistance[8]. This study leverages bioinformatics to identify oxidative stress-related genes in PCOS, such as LTA, BCL2A1, TNFSF10, NCF2, and PLA2G7, and reveals their significant associations with conditions like asthma and Type I diabetes through single-gene GSEA analysis. This underscores the necessity for advanced diagnostic techniques and targeted therapeutic strategies, informed by an understanding of oxidative stress in PCOS pathogenesis.
BCL2A1, a constituent of the BCL2 protein family, encompasses pro-apoptotic and anti-apoptotic proteins[9]. Identified as an anti-apoptotic protein, BCL2A1's overexpression in various tumor cells has been associated with cancer progression by impeding apoptosis, diminishing drug and radiation sensitivity, and reducing cellular death[10]. Within the scope of PCOS research[11], miR-664a-3p has been found to target the 3´ untranslated region (3´UTR) of BCL2A1, inhibiting its translation. Nevertheless, direct discussions linking BCL2A1 to PCOS are sparse, necessitating further investigation.
TNFSF10, belonging to the tumor necrosis factor ligand superfamily, engages with receptors DR4, DR5, and decoy receptors DCR1, DCR2, and osteoprotegerin (OPG)[12]. This engagement initiates a cascade through FADD, signaling apoptosis activation in the nucleus and catalyzing Caspase8 and Caspase3 to induce apoptosis in tumor cells[13]. In PCOS, follicular granulosa cells exhibit abnormal proliferation or apoptosis rates[14, 15], suggesting TNFSF10's involvement in granulosa cell apoptosis anomalies, though its precise role in PCOS pathogenesis warrants further elucidation.
NCF2, coding for p67phox[16], has seen its expression across varied cell types in mammals[17]. Notably, Surleen Kaur et al.[18] observed a significant upsurge in NCF2 within granulosa cells of PCOS-IR patients compared to controls. NCF2, as a crucial cofactor for NADPH oxidase, may elevate NADPH oxidase activity, inducing oxidative stress—a central factor in PCOS development. Despite the emerging evidence, the detailed mechanisms through which NCF2 mediates oxidative stress in PCOS remain underexplored, highlighting the need for additional research in this area.
PLA2G7, identified as a macrophage-derived factor in tumor biology, plays a pivotal role in the migration of various tumor cells[19]. It encodes Lp-PLA2, which interacts with low-density lipoprotein (LDL) in the bloodstream to hydrolyze phosphatidylcholine from oxidatively modified LDL, resulting in lyso-phosphatidylcholine and oxidized non-esterified fatty acids—compounds with potent pro-inflammatory properties. Traditionally recognized as a biomarker for cardiovascular disease onset, PLA2G7's levels are notably increased in unstable atherosclerotic plaques, showing a significant correlation with cardiovascular disease outcomes and prognosis[20]. Despite established connections in cardiovascular pathology, the link between PLA2G7 and Polycystic Ovary Syndrome (PCOS) has not been previously explored, presenting an innovative research avenue.
This study, utilizing bioinformatics tools, uncovered the overexpression of PLA2G7 in patients with PCOS and corroborated these findings through the development of a PCOS mouse model. The observed upregulation of PLA2G7 in PCOS suggests its involvement in the syndrome's characteristic lipid metabolism disorders and chronic low-grade inflammation, proposing a novel aspect of PCOS pathophysiology that warrants further investigation.
LTA, belonging to the tumor necrosis factor superfamily, stands as a predominant pro-inflammatory mediator and a known contributor to atherosclerosis. It operates by engaging with TNFR1 or TNFR2 receptors and is predominantly secreted by T lymphocytes[21]. As a critical pro-inflammatory cytokine, LTA's interaction with leukocytes, endothelial cells, and smooth muscle cells facilitates the induction of secondary inflammatory cytokines, including tumor necrosis factor-alpha and vascular cell adhesion molecule-1[22]. Despite its established role in inflammation, investigations into LTA's connection with Polycystic Ovary Syndrome (PCOS) remain absent. Given its potent pro-inflammatory capabilities, it is hypothesized that LTA may play a significant role in the onset and advancement of PCOS by driving inflammatory processes.
Moreover, this study's single-gene GSEA enrichment analysis of principal oxidative stress biomarkers in PCOS revealed significant enrichment in the asthma pathway for BCL2A1, TNFSF10, NCF2, PLA2G7, and LTA. This finding proposes a potential association between asthma and the development of PCOS. Supporting this hypothesis, a retrospective cohort study from 2015[23]found a higher hospitalization rate for asthma among women with PCOS (10.6%) compared to controls (4.5%), highlighting increased asthma susceptibility in PCOS patients. Similar trends have been observed in other epidemiological studies across different populations[24], with women with PCOS also receiving more asthma medication prescriptions than the general female population[25]. Additionally, DNA methylation, the process by which cytosine converts to 5-methylcytosine, affects gene expression without altering DNA sequences, responding to environmental and lifestyle changes[26]. Both PCOS and asthma exhibit abnormal methylation signaling pathways[27], possibly underlying the observed high asthma prevalence in PCOS patients. These insights, supported by epidemiological evidence and this study's biomarker analysis, underline the need for further investigation into the mechanistic links between PCOS and asthma.
Emerging literature suggests that dysregulation within the immune system, notably the imbalance between innate and adaptive immune cells, may significantly contribute to the pathophysiology of Polycystic Ovary Syndrome (PCOS)[1]. This study delves into the correlation between PCOS and immune cell anomalies via comprehensive immune cell infiltration analysis. By assessing the infiltration scores of 28 immune cell types in both PCOS patients and a healthy control group, notable discrepancies were identified, particularly in Activated CD4 T cells and Memory B cells. These findings align with existing reports indicating elevated CD4 + T lymphocyte levels in PCOS sufferers[28, 29].
Upon activation, naive CD4 T lymphocytes differentiate into various helper T cells (Th1, Th2, Th17) and regulatory T (Treg) cells, orchestrating the immune response. Th17 cells, known for producing IL-17, play a pivotal role in regulating tissue inflammation and provoking extensive inflammatory reactions[30], emerging as critical contributors to inflammatory diseases[31]. Contrastingly, studies have observed a significant reduction in the Treg cell population alongside an increase in Th17 cells in both PCOS patients and animal models[32, 33]. This Th17/Treg imbalance likely intensifies inflammation, aggravating chronic inflammation, and thereby, could be a central mechanism driving PCOS progression. Consequently, immune dysfunction and the resultant chronic low-grade inflammatory state are intimately linked to PCOS development and progression[34, 35].
{kind=link}
{kind=link}