Patients with CHF face additional challenges from social factors. The results showed that at baseline, only low support utilization increased the risk of death; however, during the course of the disease, unfavorable SDoH, low social support, and low support utilization all contributed to the death. This study is one of the few studies to comprehensively investigate the causality between SDoH throughout the course of disease and death in patients with CHF. Healthcare disparities related to SDoH considerably influence cardiovascular diseases [4]. This study provides new targets and ideas for residual risk to improve the prognosis of CHF by intervening in nontraditional risk factors of SDoH.
RCTs face significant challenges when they come to social factors, while conventional observational cohort studies often lack adequate handling of time-dependent confounders. IPW of MSM can effectively reflect the true causality between SDoH and mortality outcomes in CHF patients. Previous studies have only assessed the impact of baseline SDoH on prognosis and yielded mixed results regarding the association between SDoH and CHF. This study performed causal analyses at both the baseline and post-follow-up and corrected the effects of the time-dependent confounders. At baseline, the results showed that SDoH was not associated with death in patients with CHF, similar to a cohort study in the United States [24]. Other studies showed that unfavorable SDoH was a risk factor for death in patients with cardiovascular disease [25,26]. The research results present paradoxes because they focus solely on cross-sectional studies at baseline, neglecting the influence of confounders or improper control of confounders. In this study, CHF-PROM was regularly collected during the follow-up period, which can accurately reflect the SDoH status of patients. Secondly, most studies that focused on the SDoH were real-world studies. Inevitably, multiple confounding factors in the analysis lead to biased risk-prediction results. MSM, a well-established causal inference model, addresses time-dependent confounders in longitudinal studies. The application of MSM ensures the reliability of results [27,28]. Third, some studies only assessed the social support received by patients, ignoring their utilization, which led to an incomplete reflection of SDoH. This study also confirmed the causality between low support utilization at baseline and death. The COACH secondary study noted that patients with low support utilization displayed poor self-care behaviors, which further affected the prognosis of patients with CHF [29].
This cohort study assessed the causal effect of SDoH, social support and support utilization in patients with CHF during the follow-up period. MSM was used to analyze the data. These results showed causality between SDoH, social support, support utilization, and death. This causality may be because the patient’s SDoH and social support at baseline did not impact death. However, during the course of the disease, unfavorable SDoH has cumulatively impacted patients with CHF [30,31]. The MSM results indicated that patients with more unfavorable SDoH had a higher risk of death. Patients with unfavorable SDoH are in unfriendly social environments; thus, they receive poor social support and medical resources [32]. In addition, during the course of the disease, unfavorable SDoH cause or aggravate the negative emotions of patients, which further affects the self-management of CHF and increases the risk of death [32]. An observational study of 119 patients with CHF over a 6-year follow-up found an association between social isolation and death [33], which is consistent with our study. Our study had a larger sample size and focused on social risk factors. This study also confirmed that low support utilization by patients with CHF increased the risk of death. Higher utilization of social support plays a positive role in the self-management of patients with CHF by enhancing self-efficacy [34]. Caregivers and clinicians should prioritize patient support utilization while providing social support. This emphasis on support utilization could comprehensively reduce unfavorable SDoH and improve prognostic outcomes in patients with CHF. Overall, there is no causal relationship at baseline between patients’ unfavorable SDoH and mortality outcomes. However, the impact of unfavorable SDoH on patient outcomes is crucial for a considerable period after discharge. This finding underscores the importance of outpatient management and long-term attention to SDoH for patients with CHF. It is essential to pay more attention to patients in unfavorable social environments after discharge, as they may be more affected by various adverse factors. Furthermore, it is necessary to develop appropriate intervention strategies for risk factors associated with unfavorable SDoH, low social support, and low support utilization to improve patient outcomes.
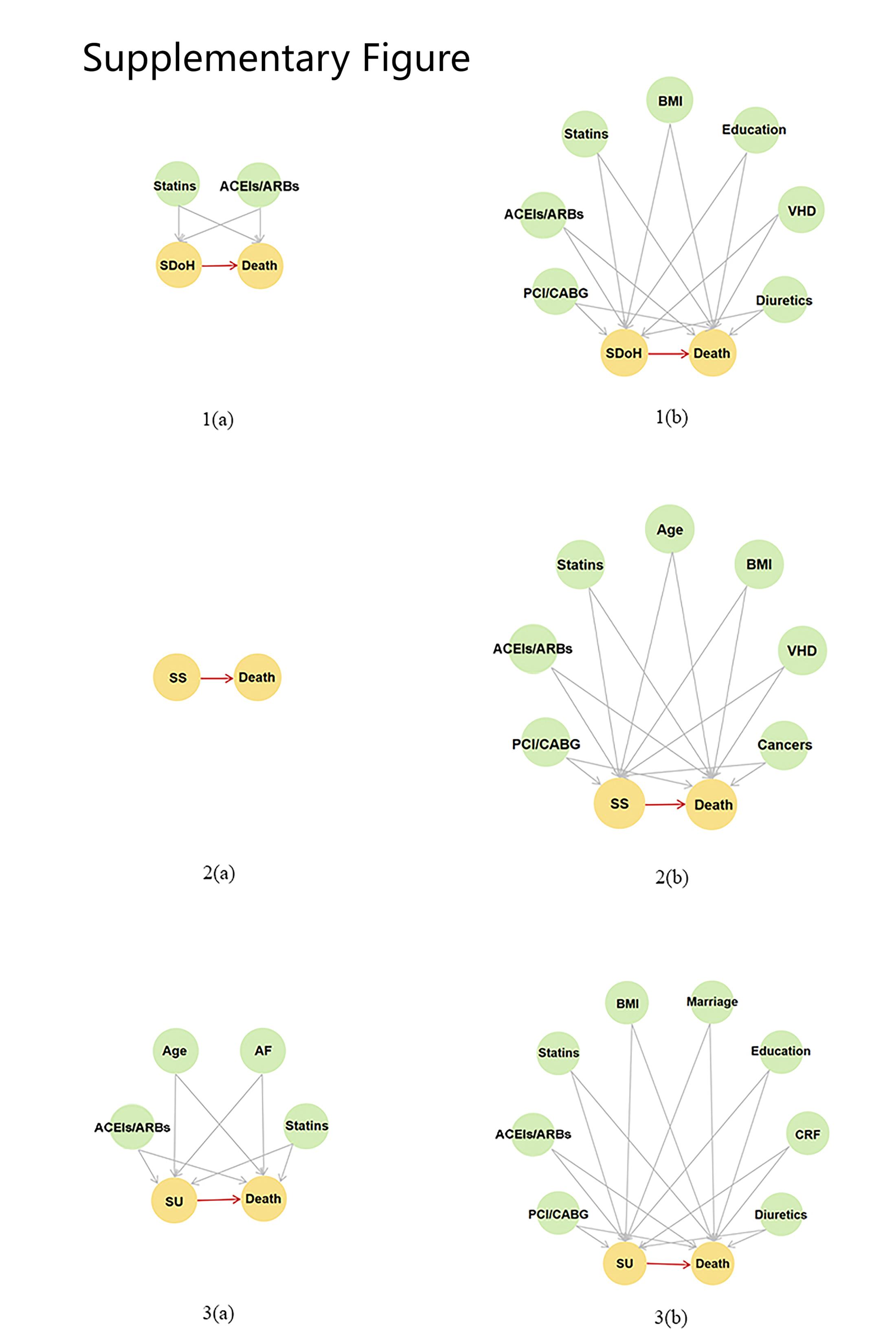
Screening for confounders associated with exposure and outcome is a critical step in MSM. In this study, the confounders identified might have been involved in mediating the causality between SDoH and mortality in patients with CHF. We found that confounders associated with all three exposures (unfavorable SDoH, low social support, and low support utilization) and death were low BMI without ACEIs/ARBs, statins, or revascularization. Confounders associated with outcomes and exposure included low BMI, low education, non-marital status, and the absence of ACEIs/ARBs, statins, or revascularization. Previous studies confirmed the phenomenon of an “obesity paradox” in CHF, viz. high BMI is associated with a better prognosis [35]. This finding is consistent with the results of the present study. BMI is associated with unfavorable SDoH in developed countries [36,37]. However, the Chinese Longitudinal Healthy Longevity Survey showed that patients with low BMI had more unfavorable SDoH [38], which is consistent with the results of our study.
Therefore, the relationship between BMI and SDoH varies across countries. Clinicians in China should pay more attention to patients with a low BMI. Our study also found that some therapeutic measures of patients affect their prognosis. Our study showed that using ACEIs/ARBs and statins improved outcomes in patients with CHF. The 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure suggests that ACEIs/ARBs improve the prognosis of heart failure.
In contrast, statins are limited to patients with coronary artery disease combined with CHF [10]. This study suggested that patients who are not taking ACEIs/ARBs or statins have a lower socioeconomic status. Patients with a low socioeconomic status have poor access to health care, less motivation, and are unable to take medications as prescribed [39].
Additionally, this study found that revascularization is an effective measure for reducing patient mortality. There is insufficient evidence regarding the role of statins and revascularization on mortality in patients with CHF [10,40]. This research indicates that necessary medications and revascularization can substantially benefit patients. A cohort study of patients with CHF at the Tyumen Cardiology Research Center confirmed that most patients who underwent percutaneous coronary intervention had higher social support [41], which is consistent with the findings of our study. The similarity in findings suggests the need for increased focus on patients who do not undergo revascularization.
Therefore, outpatient management should be implemented to reduce the unfavorable SDoH throughout the entire course of CHF and improve prognosis. For example, effective social support policies should be formulated to promote patient health education and enhance patients’ utilization of social support. In the future, longitudinal causal mediation analysis could be conducted to propose interventions with causal evidence to reduce unfavorable SDoH.
Despite the careful data collection and analysis design, this study had some limitations. First, the data in our study were primarily from the Shanxi Province of China, which limits generalizability and requires further validation in other populations. Second, 120 patients were lost to follow-up. This loss may have affected the internal validity of our results. Third, the MSM application assumed that all confounders were observed. However, unobserved confounders were present in the model.
{kind=link}