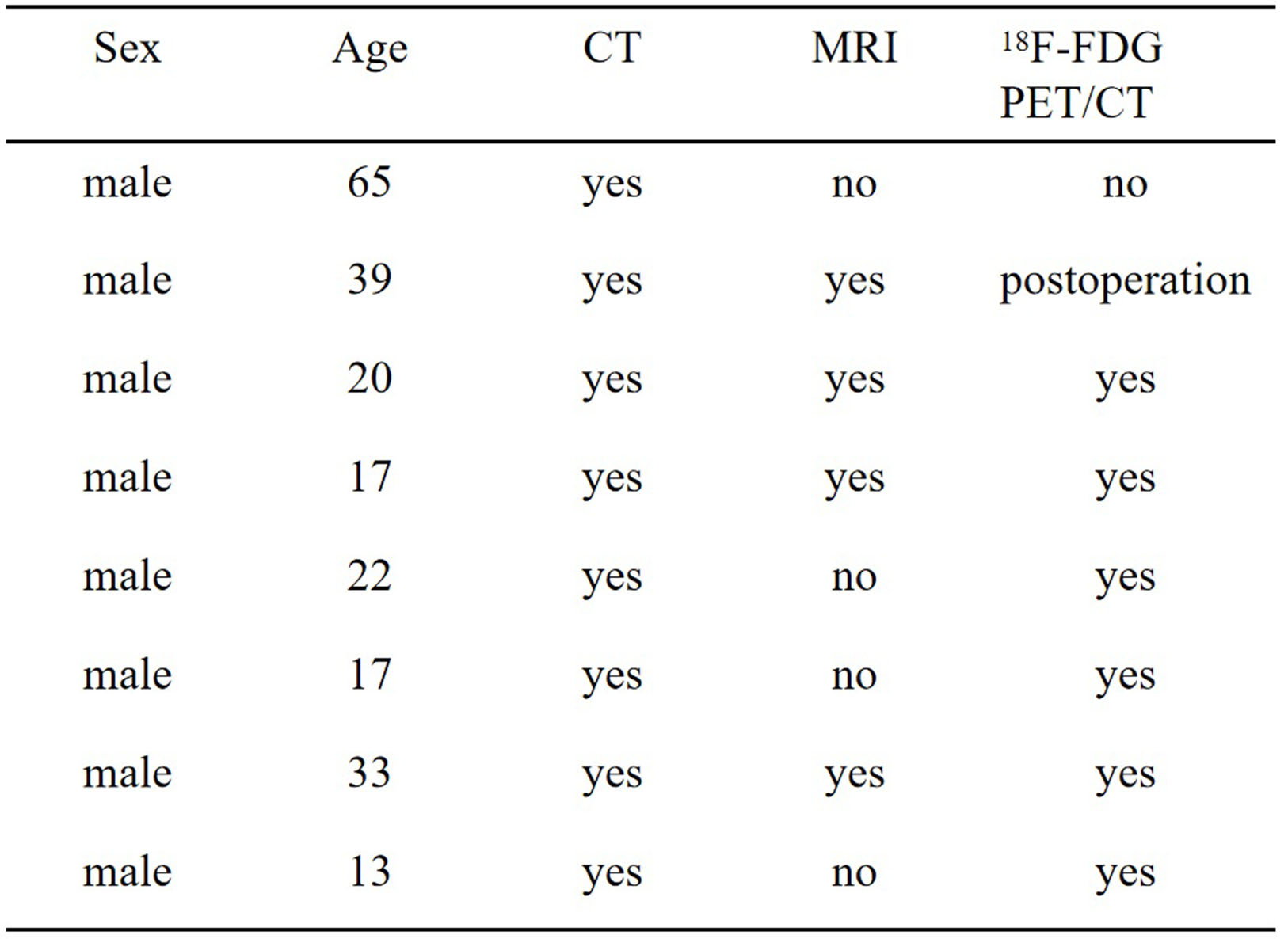
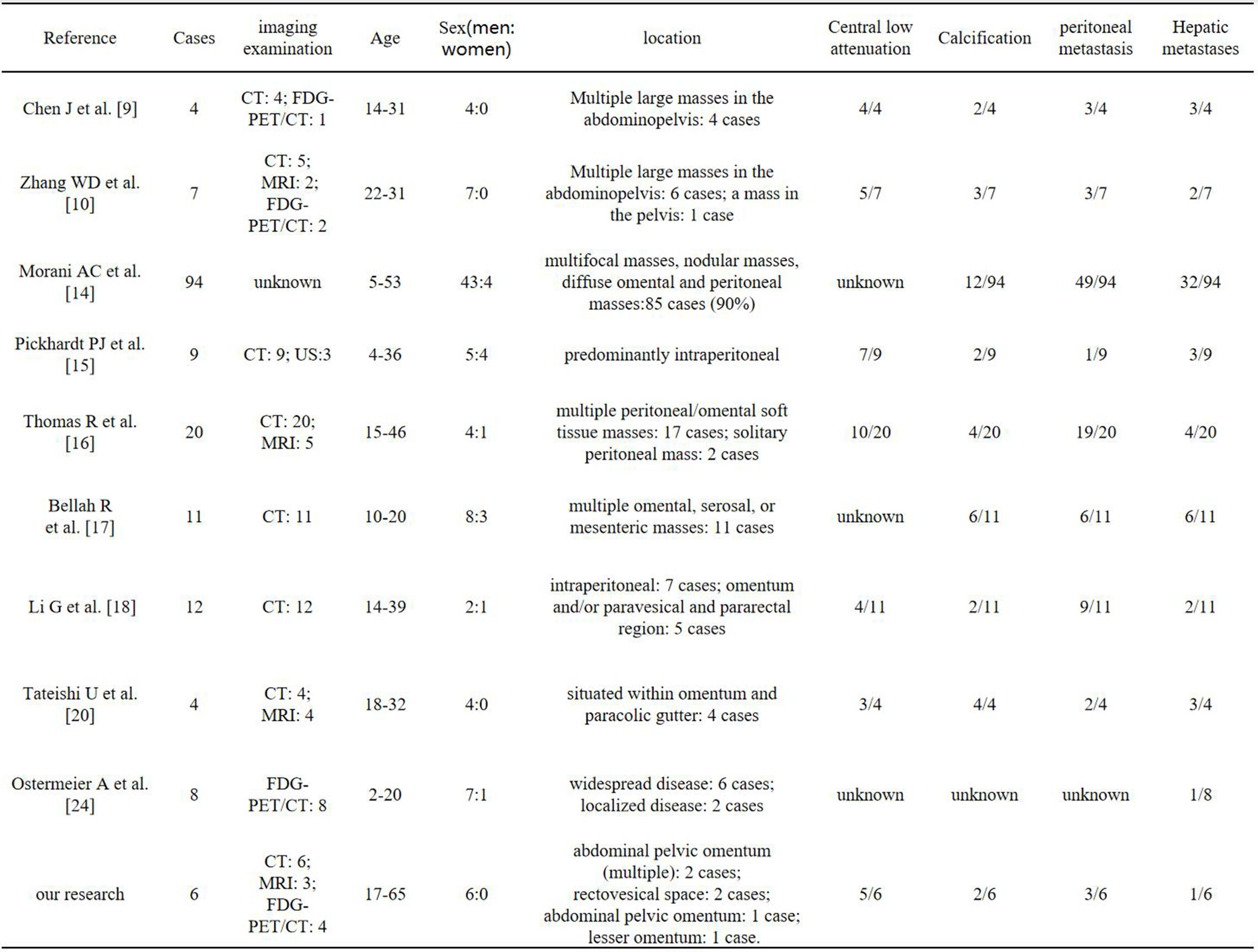
DSRCT was initially reported by Gerald and Rosai in 1989 [1]. It represents a rare malignant soft tissue tumor within the small round cell family. DSRCT primarily affects young to middle-aged males (male-to-female ratio 4–5:1) [2, 3]. Clinical presentations are often nonspecific, characterized by abdominal pain, distension, palpable abdominal masses, and may include constitutional symptoms such as weight loss and fatigue. Compression of surrounding organs may lead to manifestations like renal hydronephrosis and intestinal obstruction [2, 3, 11–14]. DSRCT commonly arises on the serosal surfaces within the peritoneal cavity and is frequently metastatic at the time of discovery. Involvement of the diaphragm and the retroperitoneum occurs in 40%-50% of cases, and liver metastases are relatively common (> 30%) [14]. Previous studies suggested a predilection for the pararectal spaces, with many cases presenting as multifocal pelvic masses. According to the imaging study conducted by Morani AC et al on 94 patients with DSRCT, 90% of the patients presented with multiple abdominal and pelvic masses [14–17]. However, our study challenges this notion, as only three cases in our cohort were located in the rectovesical space, and two cases manifested as multifocal pelvic masses. Furthermore, within our cohort, there was one case localized to the left kidney. Since Su et al.[32] first reported primary renal DSRCT in 2004, a total of 13 cases have been documented in the literature [33, 34], consistent with previous reports [33], indicating a predilection for left renal involvement in renal DSRCT. The age range in our cohort of eight patients was 13–65 years, with a median age of 21 years. Notably, one patient presented at the age of 65, surpassing the typical range of 18–25 years [16]. Cases in this age group are rarely reported in the literature. Additionally, this patient exhibited a larger tumor measuring approximately 18cm × 12cm × 6cm. Intraoperatively, we observed the tumor originating from the greater omentum, invading the midsection of the transverse colon, the anterior wall of the bladder, and the abdominal wall. No distant metastases were identified.
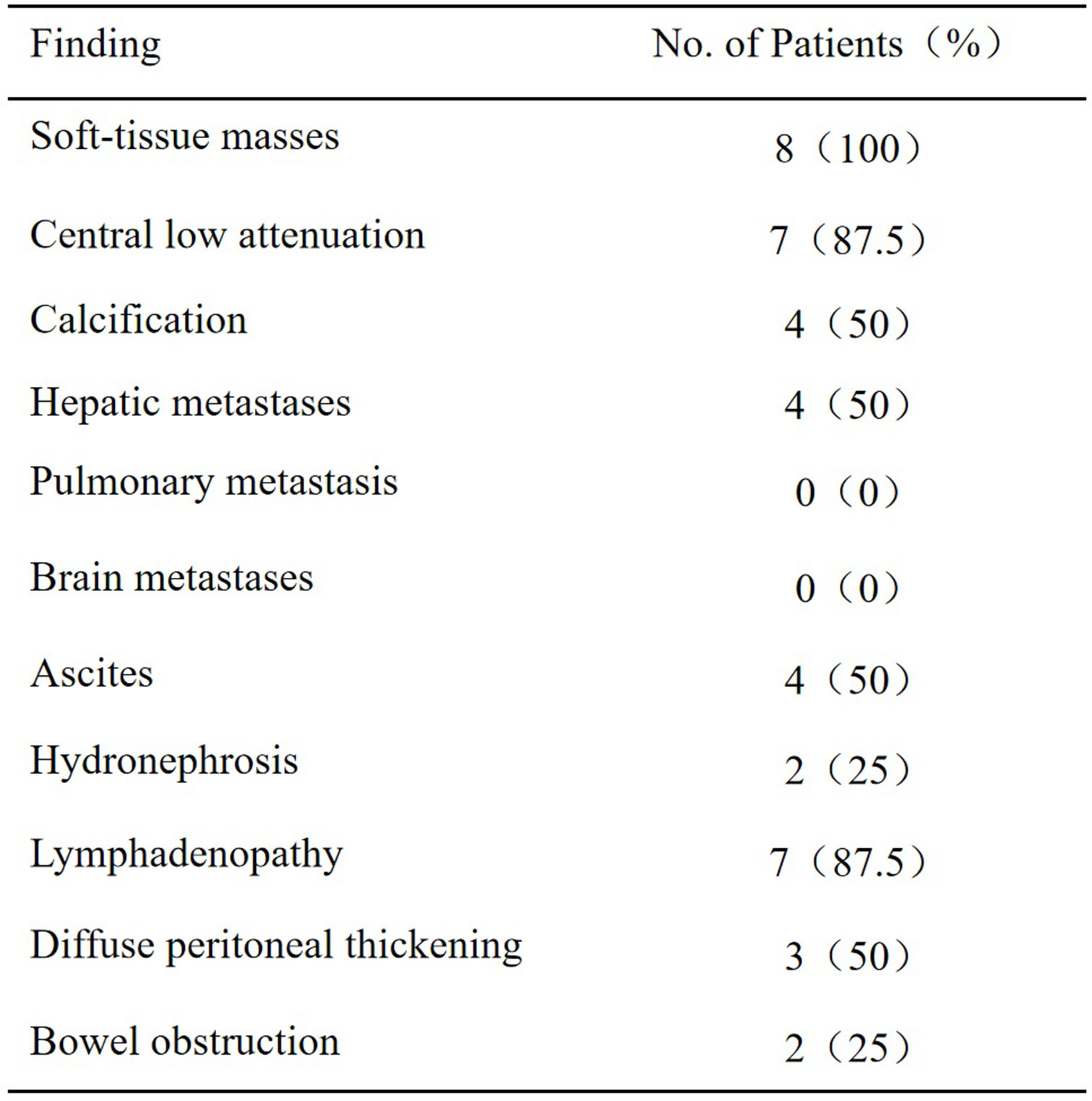
Routine imaging examinations such as CT and MRI play a crucial role in providing morphological information for patients with DSRCT, with CT being the preferred modality for diagnosis [18]. DSRCT typically manifests as solitary or multifocal lobulated soft tissue masses within the pelvic and abdominal peritoneum, lacking a defined organ of origin. Larger soft tissue masses may exhibit abnormal density changes such as necrosis, hemorrhage, or fibrous components [9]. In the study by Pickhardt et al., two out of nine patients presented with solitary masses, and seven had central low-density areas within the masses, with two showing calcifications [15]. In our research involving eight patients, six presented as solitary nodules, seven showed areas of low density within the lesions, and four exhibited calcifications.
Enhanced CT reveals mild-to-moderate enhancement in the masses, with larger masses potentially displaying peripheral enhancement [19, 20]. In comparison to CT, MRI offers unique advantages in delineating the extent of lesions and peritoneal metastasis. DSRCT typically appears as heterogeneous low signal intensity on T1-weighted images and heterogeneous high signal intensity on T2-weighted images. Multisequence signal changes in MRI contribute to characterizing the components of DSRCT [21, 22]. In our case series, seven cases exhibited central low density/signal and non-enhancing areas on CT/MRI images, possibly indicative of central hemorrhagic necrosis within the tumor [9]. However, distinct features such as T1-weighted high signal and fluid-fluid levels suggesting hemorrhagic changes were not observed in this cohort. Notably, two cases in our series presented with cystic lesions near the stomach and in the left kidney, respectively, predominantly cystic in nature, with the cystic component located away from the central tumor area. Post-contrast imaging demonstrated mild-to-moderate enhancement in the solid portion, while the cystic component showed no significant enhancement. This presentation, predominantly cystic and away from the central tumor area, is infrequently reported in previous cases.
FDG-PET/CT holds a functional imaging advantage, revealing metabolically active masses within the pelvic and abdominal peritoneum. Rosoff et al. noted changes in SUV values post-treatment in DSRCT, indicating that FDG-PET/CT can provide unique metabolic status information beyond what CT and MRI can measure. This is particularly advantageous in assessing treatment efficacy and detecting concealed lesions [16, 23, 24]. In our study, PET/CT examinations were conducted for a total of seven patients. Liver metastasis was identified in four case, multiple lymph node metastases in the pelvic and abdominal peritoneum were observed in seven cases, and one patient, during a follow-up three months post-surgery, exhibited metastatic lesions adjacent to the hepatic flexure of the colon. It is worth noting that in our cohort, there was one case with a lesion localized to the left kidney, which showed FDG-PET/CT findings of metastasis to the left renal hilum, retroperitoneal area, and para-aortic lymph nodes, as well as multiple bone metastases throughout the body. Previous reports on PET/CT findings in DSRCT involving the left kidney are scarce. These findings suggest that PET/CT, on the basis of CT and MRI, can aid in identifying the extent of DSRCT lesions, assessing systemic metastasis, and evaluating the effectiveness of tumor therapy.
In histopathology, tumor cells are surrounded by a proliferative connective tissue stroma, exhibiting a nested arrangement. The tumor cells are small in size, predominantly round or oval, with most cells having sparse cytoplasm and deeply stained nuclei. Immunohistochemically, tumor cells demonstrate multidirectional differentiation expressing various immune phenotypes, including EMA, keratin, NSE, vimentin, and desmin, among other markers [19, 25, 26]. This broad antigen expression profile is a characteristic feature of DSRCT and can be utilized to differentiate DSRCT from other tissue-related small round cell tumors [27]. Reported expression rates for the epithelial marker CAM5.2 and EMA are approximately 70% and 90%, respectively. Desmin is expressed positively in up to 72% of lesions, and its characteristic feature in DSRCT includes focal or diffuse distribution of subnuclear dots, consistent with previous literature [28, 29]. Our study results are in general agreement with the aforementioned literature. Additionally, while nearly all DSRCT cases in previous reports have shown positive expression for WT1, only two cases in our study exhibited WT1 positivity. This discrepancy may be attributed to variations in transcript variants altering the immunostaining pattern, suggesting the need to supplement both N-terminal and C-terminal regions as a form of "molecular immunohistochemistry" for identifying EWS-WT1 transcripts [27].
The differential diagnosis of DSRCT includes rhabdomyosarcoma, malignant mesothelioma, primitive neuroectodermal tumors (PNETs), lymphoma, intra-abdominal desmoid fibromatosis, and neuroblastoma. DSRCT typically occurs in adolescents, especially males, presenting as isolated or multiple soft tissue masses without a clear organ of origin, which is a characteristic feature [15, 17]. Rhabdomyosarcoma occurs in 70% of cases in children under 10 years, with about 10% involving the peritoneum. Compared to DSRCT, rhabdomyosarcomas typically have smaller tumors and almost no calcifications[30]. Malignant mesothelioma is rare in patients under 20 years, often accompanied by pleuroperitoneal effusion, possibly related to asbestos exposure [31]. Peritoneal leiomyosarcoma is more common in females over 24 years, and PNETs are highly invasive tumors that predominantly affect young individuals. Unlike DSRCT, PNETs exhibit fewer calcifications. Lymphoma is common in middle-aged males and is characterized by thickening of the intestinal wall, enlargement of organs such as the liver and spleen, and lymph node enlargement. Additionally, calcifications and peritoneal nodules are less common in lymphomas. Intra-abdominal desmoid tumor is a rare benign fibrous tissue proliferation that predominantly occurs in females. It can occur as an isolated entity or be associated with Gardner syndrome. Compared to DSRCT, desmoid fibromatosis rarely undergoes necrosis or cystic changes and does not metastasize. Neuroblastoma is another differential diagnosis, with onset typically before the age of 5, usually presenting as a single paravertebral mass, making it easier to differentiate from DSRCT[9, 14, 19].
{kind=link}
{kind=link}
{kind=link}