In this study, 2 out of 5 patients were at their first and second recourse, respectively, and the others were at their third or more recourse. In first intention, about two-thirds of patients have used the conventional modalities and quarter within 24 hours onset of the symptoms. Then taken individually, self-medication was the main modality used first intention. The health districts in the natural regions of Middle Guinea and Upper Guinea were at risk factors of the early and appropriate care-seeking for children under five and those 5 years and over. Although progress has been made in the management of malaria cases, these results show the need for a more specifics approach in health districts to improve for early and appropriate care-seeking and reduce to the severe malaria forms. Previous studies of care-seeking behaviors in endemic countries in sub-Saharan Africa report high prevalences of self-medication in first line. These observations made in different countries show the need to expand the malaria diagnostic package to licensed drug sellers and pharmacies.
Regarding early care seeking, we find that almost half of patients have made an early use and about one third patients have made an early and appropriate recourse. Among under five group, the early and appropriate seeking was 33.66% CI95% 30.92%-36.51%. In 2021, the survey on malaria and anemia indicators in Guinea reported an early seeking-care of 32.00% among children under 5 years old [8]. A study carried out in Burkina Faso and published in 2022 as part of a pilot project shows an early and appropriate care seek of 65.5% (95% CI 63.9–68.9%) in the general population [25]. Other studies show similar prevalences, 30.4% in children under 15 years of age with simple malaria in Uganda in 2018 [26], 38.0% in Liberia in 2018 among children under five years old [27] and 18.6% in a health facility in Nigeria's Imo State in 2019 [28]. However, it is important to note that several studies use the 24–48-hour as a reference for the earliest time sought care and in this case the proportions of early seeking are higher. On the other hand, studies conducted in the context of pilot projects to improve conventional care-seeking may show higher trends.
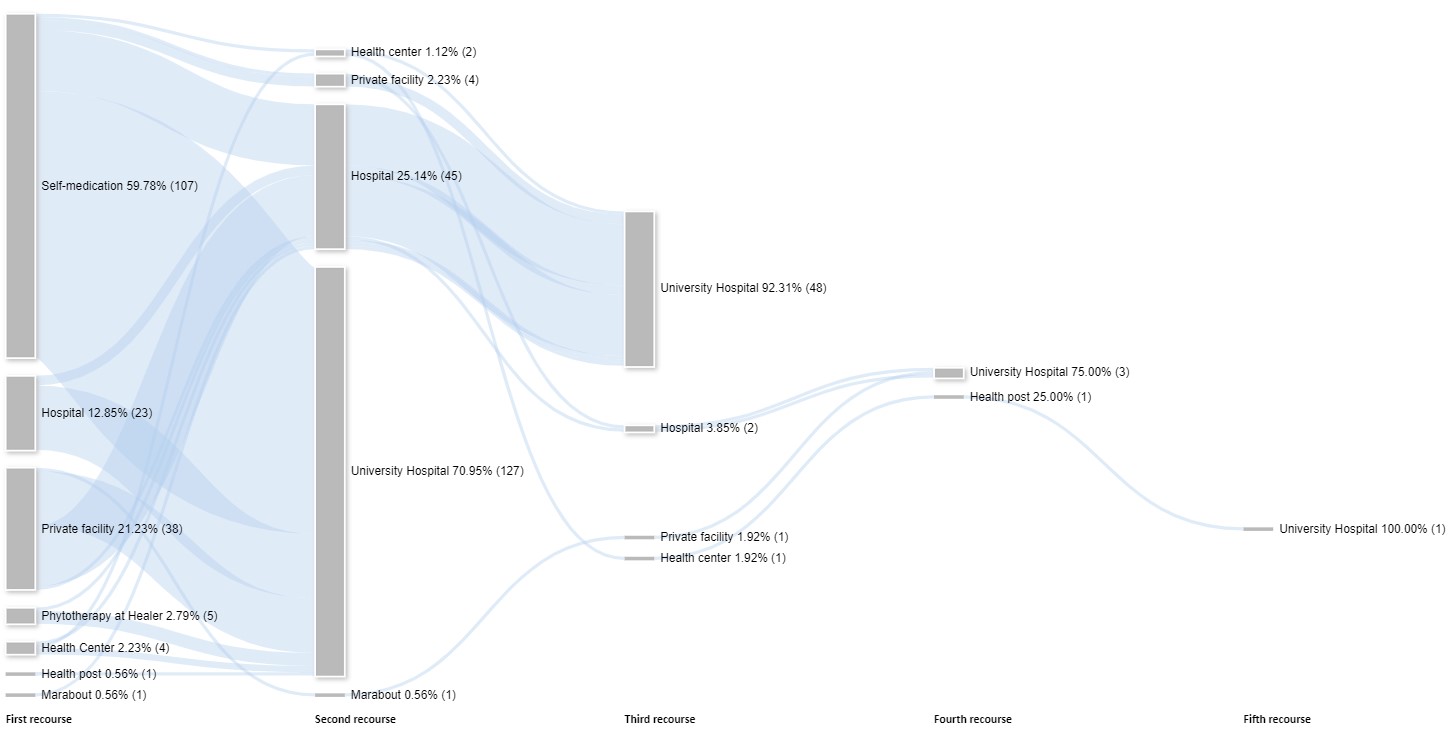
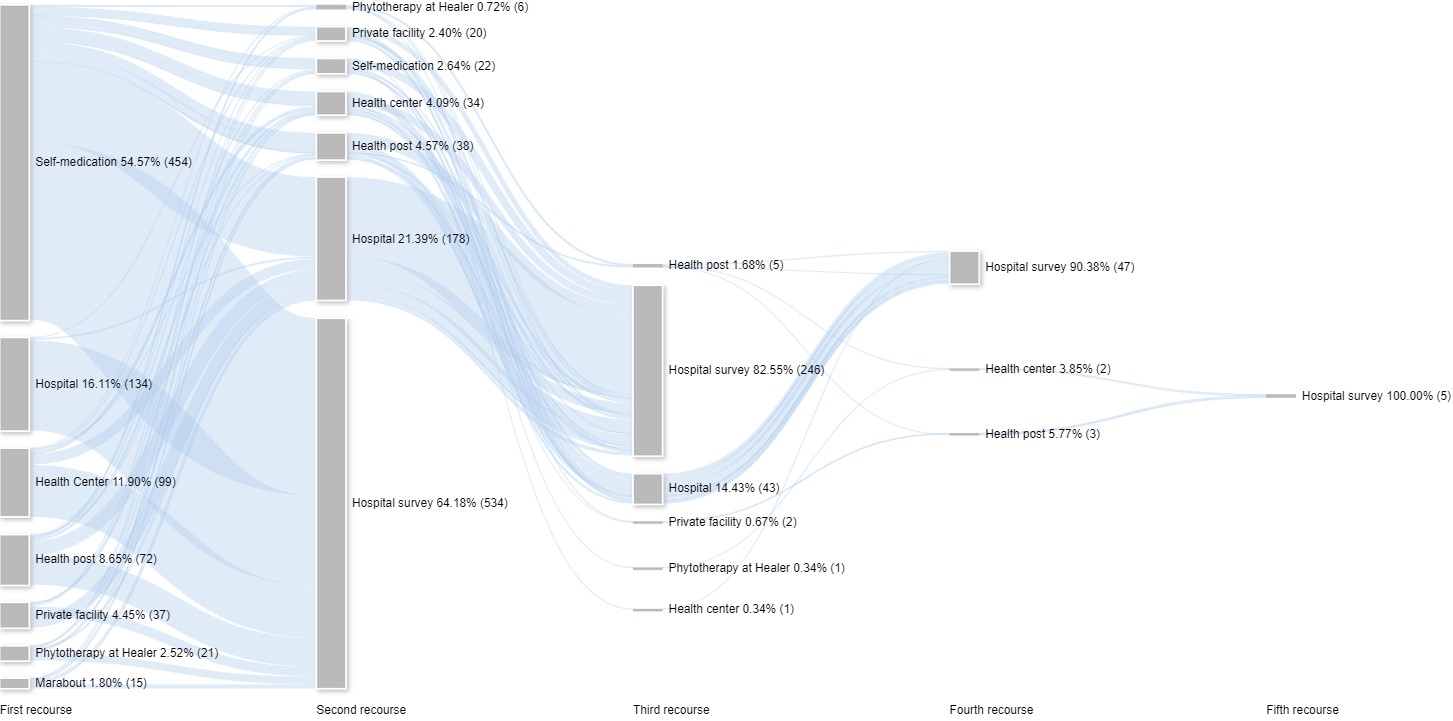
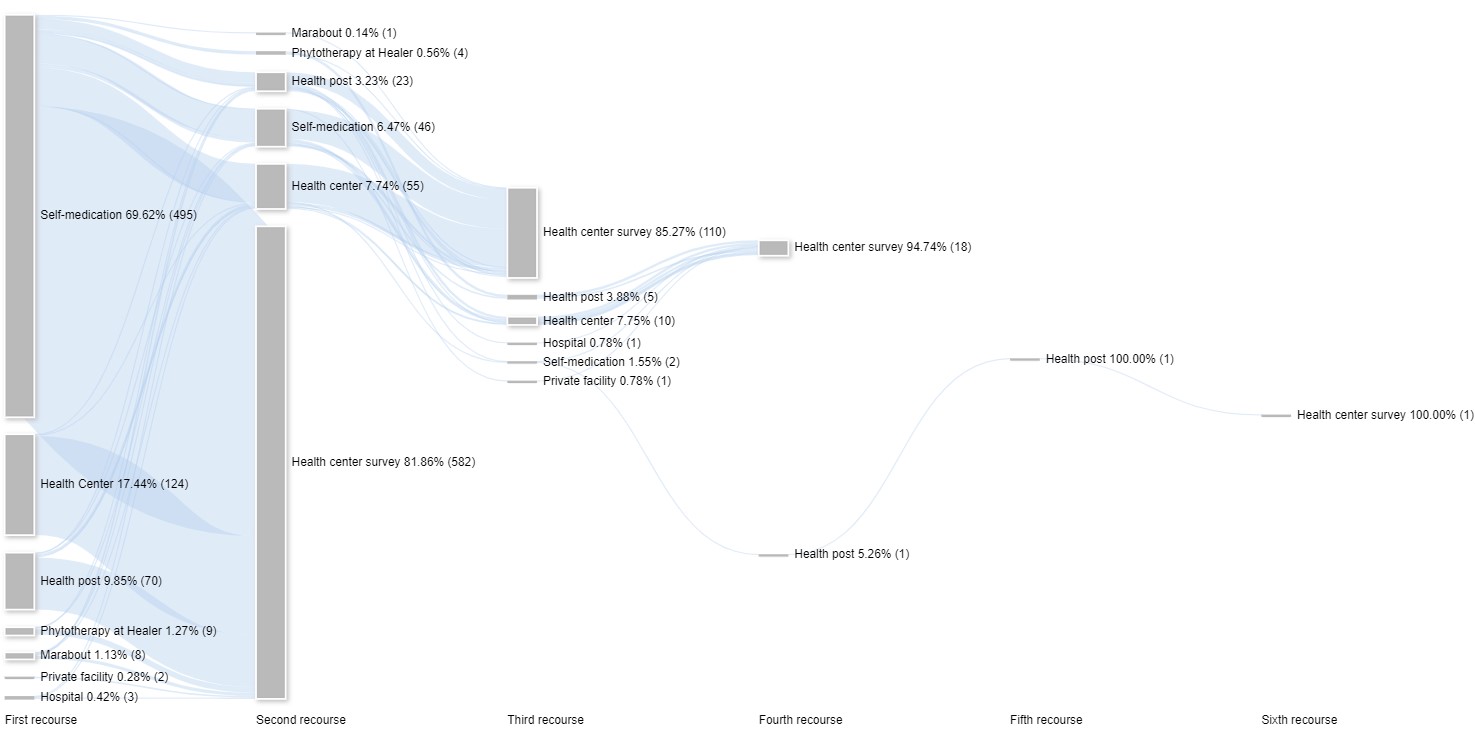
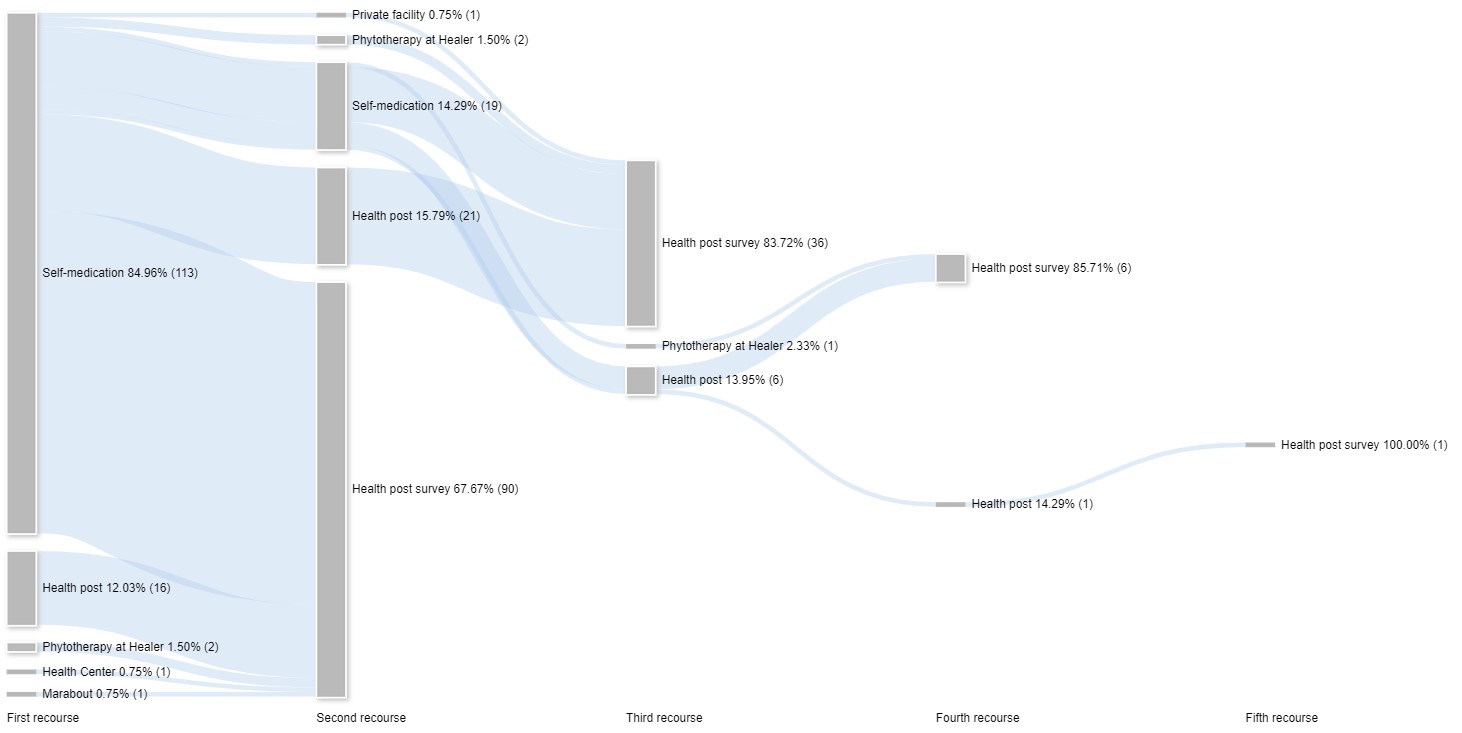
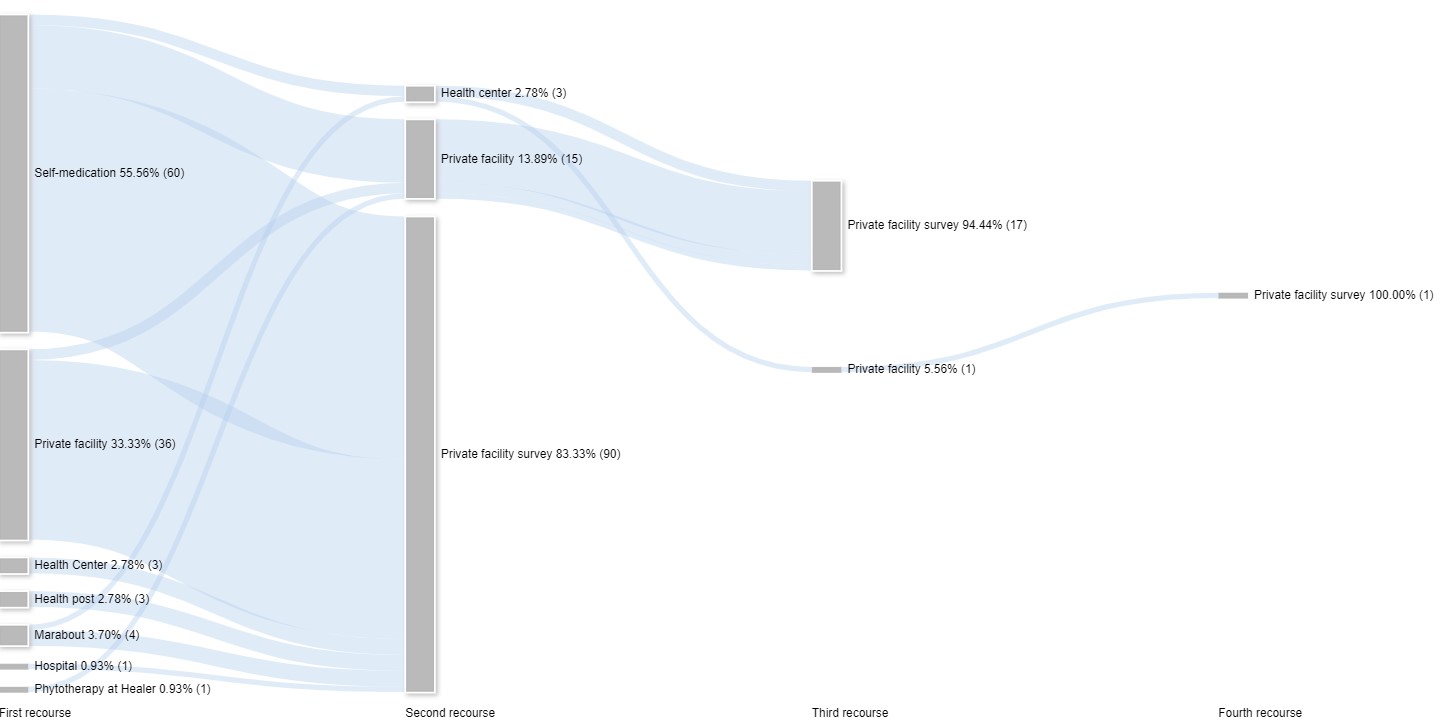
About two out of five patients said they had made only one recourse, the one at the time of the survey, and the others two or more recourse. In a study conducted at Coyah District Hospital in 2019, the maximum number of appeals made by a patient was three [29]. In Equatorial Guinea, in a study published in 2015, patients who started treatment at home had made a maximum of three recourses and those in health facilities had made two recourse, including a small proportion of those who had started treatment at home in rural areas [30]. In our study with Sankey's alluvial diagrams, we observed the complexity of the patient trajectories encountered in hospitals and health centers. This complexity can be explained by the forms of malaria admitted to these health facilities with recourse already made elsewhere (mainly self-medication), the poor quality of care and, to another extent, the lack of adherence to treatment. This observation of successive recourses to the conventional facilities calls into question the quality of malaria case management in healthcare facilities. A study carried out in Nigeria and published in 2014 shows that 45.5% of children under 5 years old used informal source of care in first line (drug sellers) [31]. Regarding self-medication as a first-line modality, some studies report similar trends with 33.5% in Kaduna State in Nigeria in 2020, Burkina Faso 34.2% in 2016 and Zambia 41% CI95% 36–46% in 2016 [32–34]. Other studies report higher trends of self-medication as the first-line treatment for fever or malaria, sometimes reaching 86.00% [35]. Using self-medication on first intention can be explained on the one hand by over-the-counter access to antimalarial and antipyretic drugs, the recognition of the signs of malaria (fever + asthenia = malaria) and the experience of a malaria attack treated by a health care provider using the available drugs. Second-line self-medication was identified in our study. Some studies report the use of self-medication as a second-line treatment, with 54.4% for simple forms and 33.7% for severe forms in Mali in 2005 and 14.8% in urban areas in Bata, Equatorial Guinea in 2015 [30, 35].
Factors associated an early and appropriate care-seeking in children under five were geographical area, monthly income of the head of household, number children under five, and suspected disease and perception of disease severity. In our study, the level education of caregivers was not associated with the early and appropriate care-seeking, this situation can be explained by the fact, the communication activities, not evaluated in this study, are carried out in the local languages of the country and are therefore accessible to most communities. Regarding the monthly household income, study based on population survey data from 16 countries in sub-Saharan Africa and published in 2022 shows that increasing one unit of women's social and economic empowerment increased the likelihood of early and appropriate seeking care for children under 5 years of age by 32.00% [36]. In addition, another study carried out in Uganda and publish in 2018 showed the socioeconomic position of the household have associated with early and appropriate care seeking (p = 0,002) [26]. Our study shows, the suspicion of teething in children increased the likelihood of seeking early care in a health facility. This result can be explained by the desire to resolve the symptoms associated with teething. The perceived severity of the child's illness was associated with delayed care-seeking in our study, OR = 0.56 95% CI 0.42–0.74 (p < 0.001), like the results of a study conducted in Uganda and published in 2009 where tachypnea in febrile children had an OR = 0.75 95% CI 0.61–0.93 [37].
Among the group aged five and over, who were the majority, the factors associated, care-seeking earlier and appropriate were the health districts Boffa (Lower Guinea, costal region) and Dabola (Upper Guinea, savanna region). The patients in these districts were at risk of delaying seeking care at health facilities or with community health workers. It should be noted that these are areas with moderate malaria transmission with seasonal trend and preventive strategy specially in Dabola (Seasonal malaria chemoprevention). A study conducted in Ethiopia and published in 2017 among children aged 2 to 9 years old shows that the intensive deployment of preventive strategies and the reduction of the transmission rate reduces the use of health facilities [38]. Our study shows that having a monthly income was positively associated with care-seeking earlier and appropriate (p < 0.001). The availability of a daily income encourages investment in appropriate health care. Studies carried out in Ebonyi State, published in 2021, and Imo State, published in 2019, Nigeria, show that mothers with employment (daily income guarantor) were quick to seek conventional care in children [39, 40].
Overall, studies to discuss our results have been identified and the originality of our approach lies in the analysis of the factors associated with the early and appropriate care-seeking (combinate variable) and the visualization of these to assess the succession of recourse to care. The detailed descriptive analysis of first-line treatment was discussed with results from studies carried out in sub-Saharan Africa while showing the place of self-medication as a first-line treatment.
Limitations
We conducted a cross-sectional study, which collected data after malaria diagnosis in health facilities. Some elements of the care pathway, including adherence and the result of the treatment, were not addressed. In addition, the history of the journey was based on the statements of patients or caregivers. And on the other hand, patients who did not present themselves at a health facility or at community health workers were not interviewed. These are the main limitations of this study.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}