Laparoscopic surgery for endometrial cancer has many advantages because it is minimally-invasive, and the oncologic outcome reportedly is not inferior to that of open surgery [3,13]. Presently, laparoscopic surgery is becoming a gold standard procedure for endometrial cancer instead of open surgery.
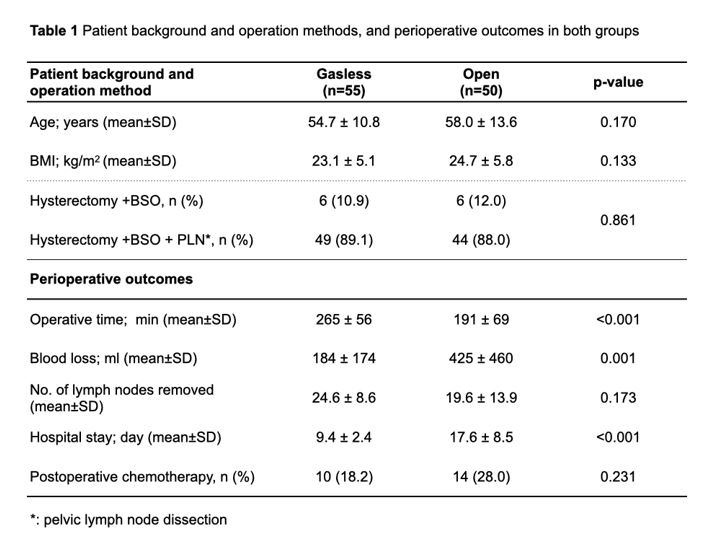
On the other hand, the effects of the pneumoperitoneum on malignant tumors, such as port site metastasis, remain unknown [14–16]. In addition, pneumoperitoneum may adversely affect heart and respiratory diseases. In such cases, GLS without pneumoperitoneum may be considered a surgical option. GLS reduced blood loss, shortened hospital stay, and reduced complications compared to open surgery. Since this was the same result as that achieved by conventional laparoscopic surgery with pneumoperitoneum [17,18], GLS may be useful as a minimally-invasive procedure for endometrial cancer.
In GLS, the surgeon is forced to operate in a narrower operative field than with conventional insufflation. Therefore, we attempted to compensate for this deficiency by using a steep Trendelenburg position (30°) and a uterine manipulator. With this approach, we were able to perform surgery without much concern about intestinal tract interference with the operative field. On the other hand, since GLS results in no operative field disorder due to abdominal collapse caused by gas leakage, surgical procedures, such as lymph node dissection using an ultrasonic surgical aspirator, vaginal wall incision for hysterectomy, removal of the uterus from the vagina, and vaginal stump suture, were performed easily in a stable operative field. These procedures are difficult to perform when the pneumoperitoneum method is used, and this is considered an advantage of GLS.
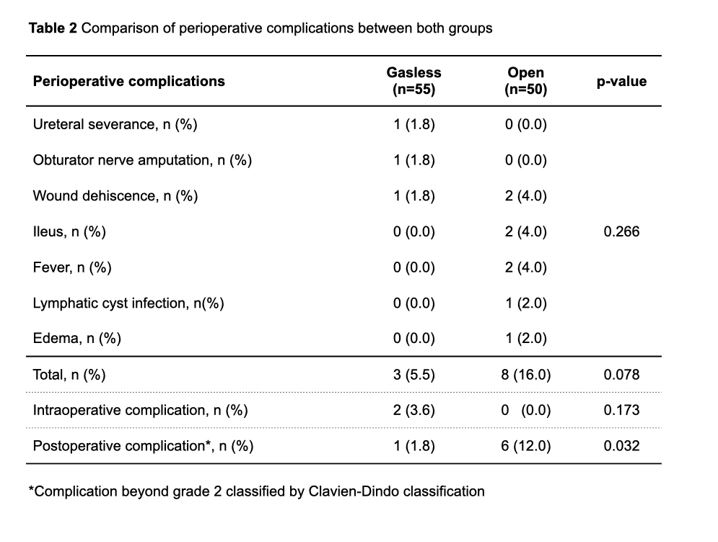
Complications in the GLS group were significantly less than those in the open group, but this probably was due to less postoperative ileus and wound dehiscence as reported in laparoscopic surgery using pneumoperitoneum [19]. On the other hand, two cases of intraoperative complications were observed in the GLS group. These were believed due to inexperienced forceps operation in the initial introduction stage.
Regarding use of the uterine manipulator, there are two contradictory reports: in one report, intraperitoneal tumor cells increased due to contact between the manipulator and tumor [20,21]. and in one the tumor cells did not increase [22,23]. However, use of uterine manipulators reportedly had no effect on oncologic outcomes [24,25].
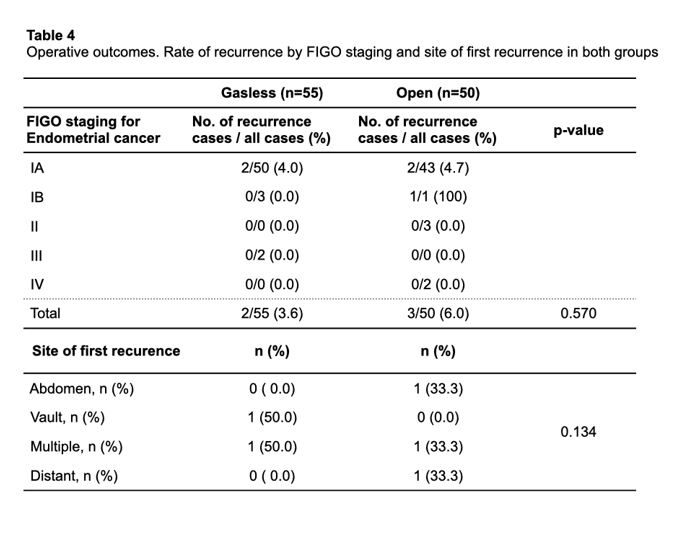
In our study, we showed statistically that use of a uterine manipulator did not affect recurrence or survival rates. However, since the average observation period was as short as 41 months, a longer observation period is necessary in the future.
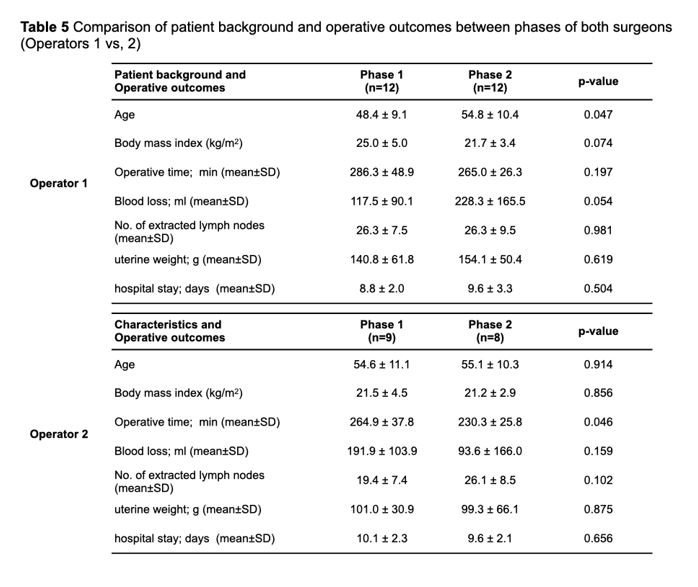
GLS has been reported to be more proficient for beginners than the conventional laparoscopic surgery using pneumoperitoneum [26]. The proficiency of GLS by two surgeons using CUCUM analysis was recognized as a biphasic learning curve with two phases: a positive slope (phase 1, representing the initial learning curve) and a negative slope (phase 2, representing the mastery phase that shortens operative time) [27,28]. The turning points changing from phases 1 to 2 were found in the early cases before and after the tenth case in both operators. In particular, Operator 2, who was not accustomed to laparoscopic surgery, showed a significant reduction in operative time in phase 2, which indicated that GLS is easy to learn even for beginners in laparoscopic surgery. On the other hand, the fact that Operator 1 showed an operative time shorter than the average operative time from the beginning of phase 1 is probably because Operator 1 was sufficiently familiar with laparoscopic surgery. The positive slope after that time is presumed to be the result of trial and error in pursuit of a more reliable procedure as he became used to the technique.
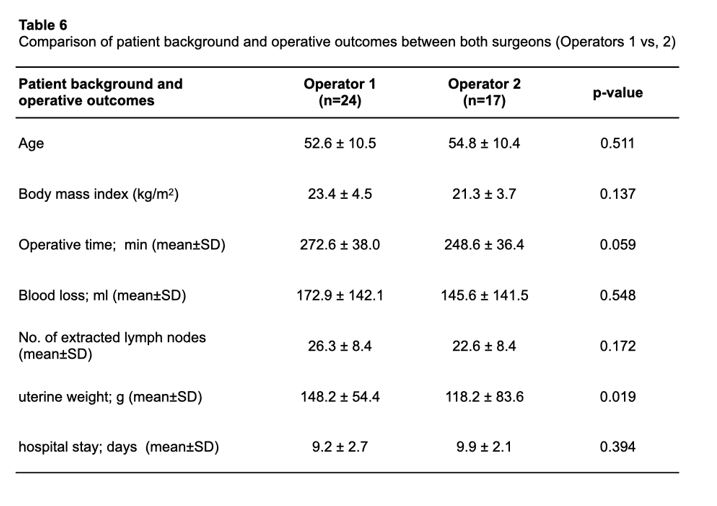
In the comparative study between two surgeons, one a laparoscopic surgery expert and one a beginner, there was no significant difference in operative time, blood loss, and number of lymph nodes removed. We speculated that the proficiency level of laparoscopic surgery does not affect the learning of GLS. The significant difference in weight of the removed uterus between the two surgeons may be attributed to the fact that Operator 2 was a novice to laparoscopic surgery and, thus, technically avoided a large uterus.
In GLS, the surgeon can perform operations similar to those during open surgery using forceps. Thus, GLS has the advantage of easily performing procedures, such as lymphadenectomy and suturing of the vaginal stump. We believe that this factor makes it easy for beginners to learn laparoscopic surgery. Our study showed that GLS has a high proficiency even with highly difficult laparoscopic methods if the surgeon is sufficiently proficient at open surgery.
However, this study has some limitations. First, we relied on the experience of two surgeons rather than the results from evaluations of many surgeons. Next, when comparing the results of the two surgeons, no consideration was given to the port size. Unlike with a conventional pneumoperitoneum, in GLS, multiple forceps can be inserted and operated from one port, so the difficulty of surgery increased if the port size was small. Since Operator 1 had abundant experience with laparoscopic surgery, the port size was set as small as possible in consideration of cosmesis. Therefore, it is undeniable that there is a bias in the difficulty of their surgeries. In this study, there was no difference in patient background between the two phases, but If there is a difference in surgical difficulty depending on the case, the operative time may be biased and the learning curves of both may be affected.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}