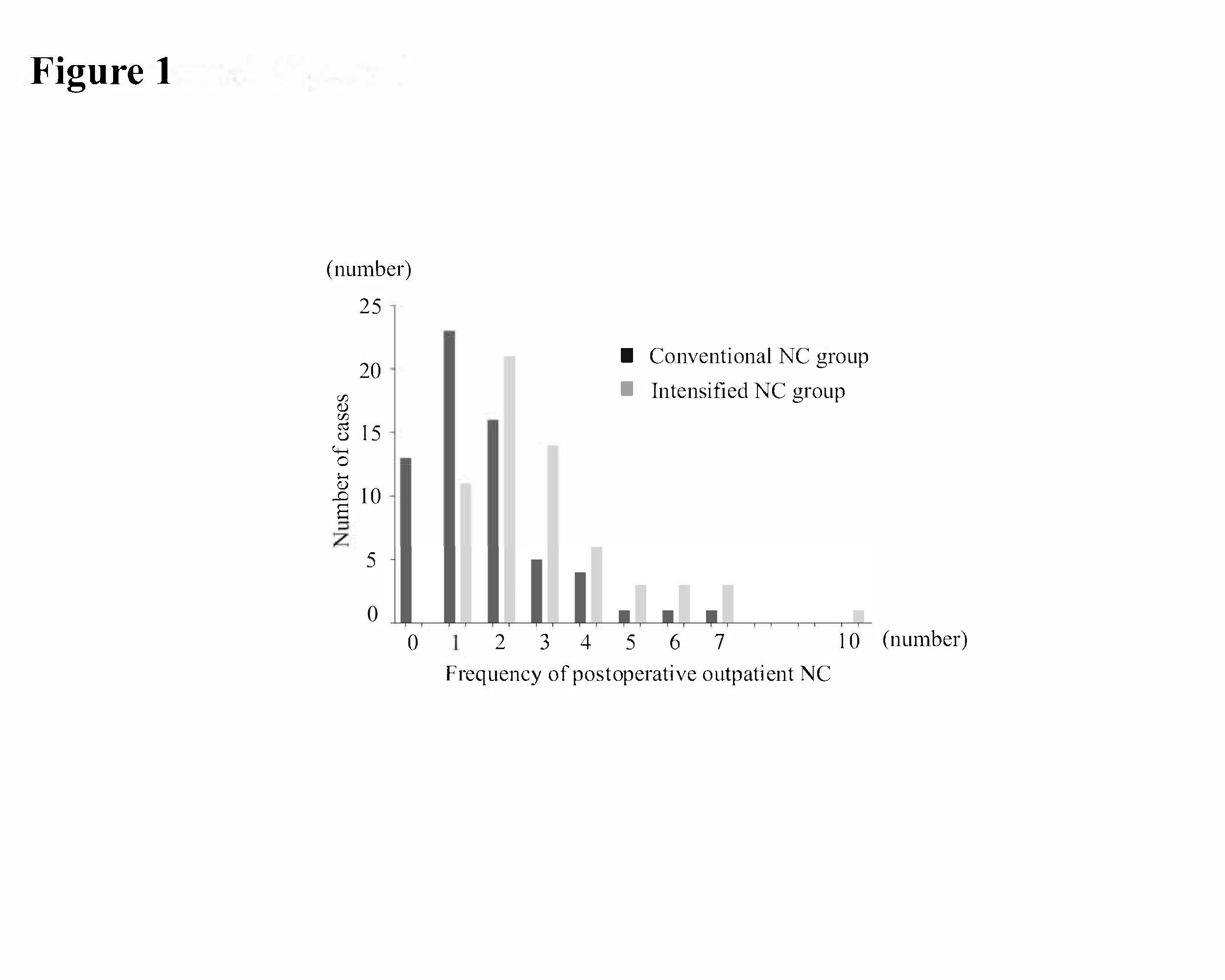
In the present study, we explored whether more intense NC contributes to an improved nutritional status after esophagectomy. From our results, iNC, in which NC was provided more frequently and continued after enteral feeding completion, could significantly reduce body weight loss and SMI loss 3–6 months after esophagectomy. Although the differences at 1 year were not significant, iNC may mitigate nutritional deficiency, leading to improved patient quality of life and outcomes.
In general, body weight loss after esophagectomy is one of the most important postoperative sequelae, and it has been reported that more than half of patients lose more than 10% of their initial weight at 6 months postoperatively [1, 10–12]. Post-esophagectomy patients often have several postoperative symptoms such as eating difficulties, pain, fatigue, nausea, and appetite loss, resulting in long-lasting weight loss after surgery [13]. Although no fundamental countermeasures for this issue have been found, enteral feeding support via enterostomy is frequently used, and ONSs and postoperative outpatient NC are provided in many facilities.
Previously, it was suggested that enteral feeding immediately after esophagectomy could suppress weight loss at 14 days postoperatively [14]. However, it has also been reported that weight loss following esophagectomy occurs once tube feeding is stopped, independent of the time interval after esophagectomy [15]. Moreover, the routine placement of a feeding enterostomy did not result in the improvement of weight loss 3 months after surgery [16]. In addition, Hyltander et al. suggested that artificial nutrition after major surgery including supportive enteral and parenteral nutrition, was not superior to oral nutrition only when guided by a dietitian [17].
Although few studies have demonstrated the significance of ONSs in post-esophagectomy patients, a recent small pilot study showed that additional ONS intake for 4 weeks after esophagectomy could prevent body weight loss at 3–6 months postoperatively, and have a positive impact on quality of life 1 month after surgery [18]. Meanwhile, a recent randomized controlled trial of patients with gastric cancer undergoing gastrectomy showed that administration of ONS for 12 weeks after gastrectomy could improve body weight loss at 3 months postoperatively, although it could not improve body weight loss 1 year after gastrectomy [19]. We could not evaluate the significance of ONS in the present study, due to its retrospective nature, as intake volume was not assessed. However, ONS may be effective in improving daily energy intake and mitigating mid-term body weight loss after upper gastrointestinal cancer surgery.
Our study showed that iNC could improve body weight and SMI loss 3–6 months after esophagectomy. RDs can provide detailed NC on diet and food intake based on a patient’s symptoms. Therefore, patients intensively guided by RDs can consume normal food supplemented with various ONSs. In addition, RDs can flexibly modify the type of ONS and diet depending on the patient’s condition and preferences. It has been also suggested that preoperative NC could preserve body weight in patients with esophageal cancer [20, 21]. Prolonged postoperative NC may improve energy and protein intake, and minimize weight and skeletal muscle loss.
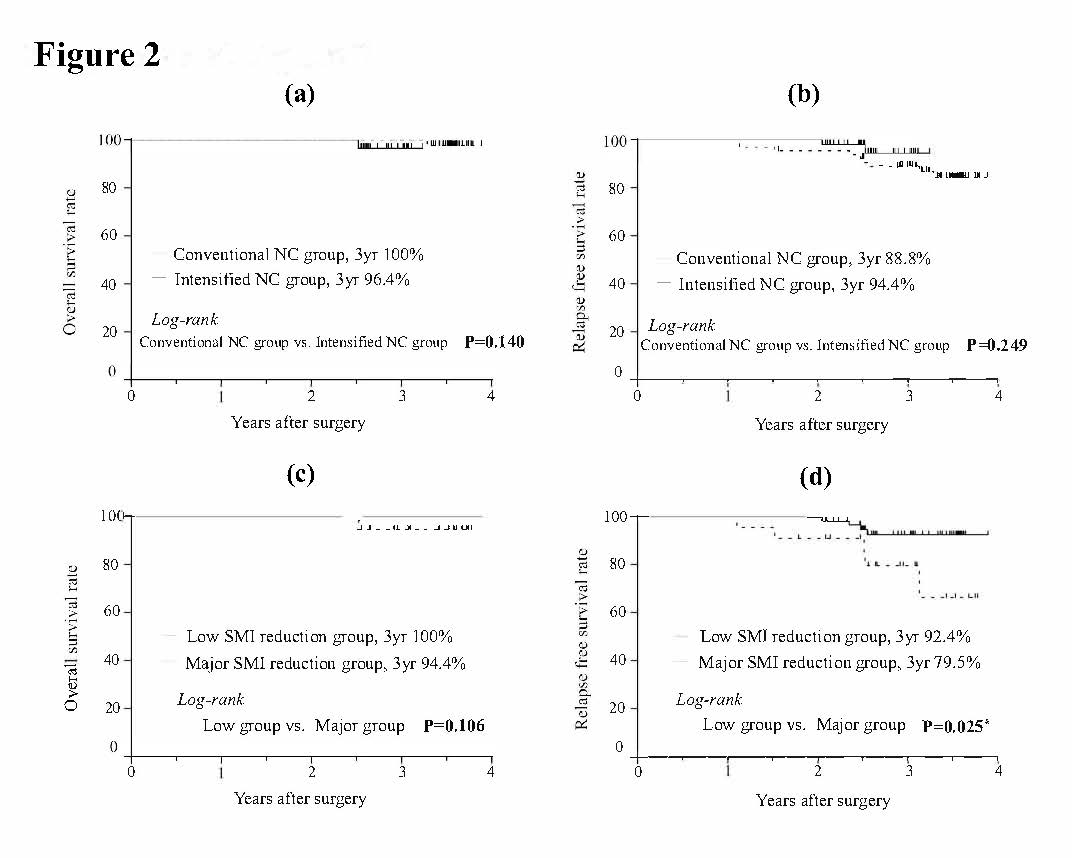
Poor nutritional status and massive reductions in postoperative body weight and SMI are significantly correlated with poor prognosis [5, 10, 13, 22]. In the present study, we also confirmed that patients with major SMI reduction had a worse prognosis than those without. However, we did not observe a significant improvement in prognosis with iNC, although iNC significantly improved body weight and SMI loss 3–6 months after esophagectomy. Since we aimed to evaluate the nutritional status and changes in body composition after esophagectomy in this study, patients who experienced disease recurrence within 1 year after surgery and those who underwent adjuvant chemotherapy after surgery were excluded. This may have influenced survival analysis.
This study had some limitations that should be addressed. First, this was a retrospective observational study conducted at a single center with a limited number of patients. Second, although the study period was relatively short, the treatment and management of the patients improved with each passing year, suggesting that it is not beyond historical comparison. Third, NC was conducted using several RDs, which may have led to differences in NC content. The analytical method used in this study may have resulted in some biases, as described above. Finally, we could not evaluate long-term quality of life. Further prospective studies assessing larger numbers of patients are required.
In conclusion, outpatient iNC significantly improved body weight and SMI loss 3–6 months after esophagectomy. Therefore, iNC may improve patients’ quality of life and outcomes by improving their postoperative nutritional status.
{kind=link}
{kind=link}