Myelination typically progresses from the chiasm to the optic nerve from the eighth month of gestation until birth and then stops at the lamina cribrosa.[1] The pathophysiology of MRNFs remains unclear. Several factors, such as the structure of the lamina cribrosa and plasma proteins, have been proposed to inhibit myelination in the normal human retina.[11, 12] MRNFs are usually present unilaterally in most cases.[5] Previous studies have reported the potential progression of these lesions[3, 13]; their findings on autofluorescence, fluorescein angiographic images,[12] or OCT[13]; and their natural history.[13] With the advent of new examination equipment, doctors have more means of gaining a deeper understanding of such diseases. The present study is the first to investigate the fundus using true-color, ultra-wide-field fundus images and OCTA metrics, and to identify the associations among the area and location of MRNFs with myopic parameters and OCTA metrics.
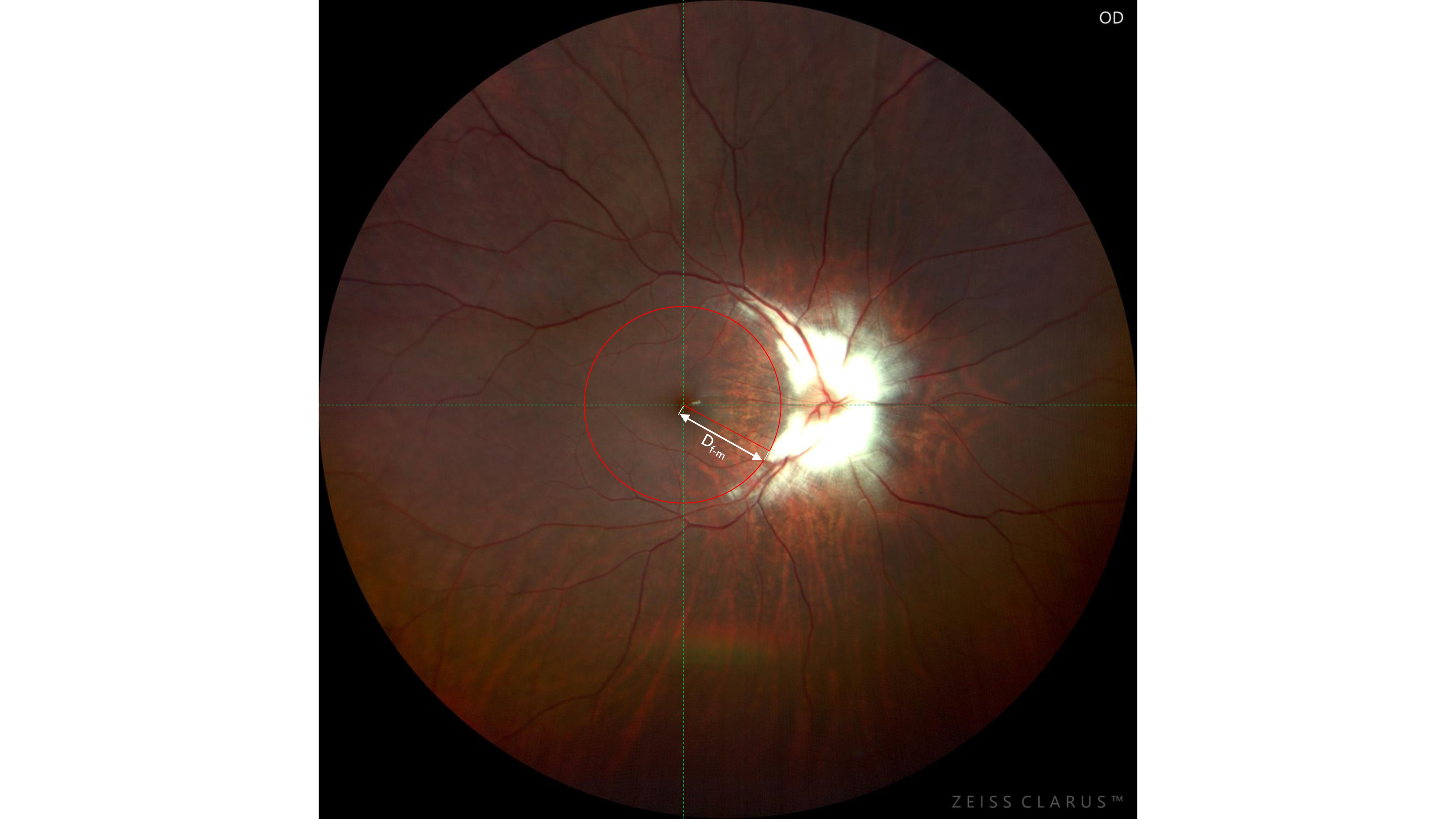
In this study, eyes with MRNFs exhibited poorer CDVA compared to control eyes matched for age, SER, and AL. MRNFs are often associated with high myopia, anisometropia, and amblyopia. Vision loss may occur due to anisometropia and amblyopia, or secondary to structural abnormalities of the retina and/or optic nerve.[1] In accordance with our study, Kee et al.[14] investigated the visual prognosis of amblyopia associated with anisometropia and MRNFs in 12 children (mean age: 4.2 years, range: 2.1–8.6). They found that the amount of anisometropia and the area of myelination differed between groups with different CDVA. In addition, our study found that CDVA was strongly positively correlated with the area of MRNFs and negatively correlated with Df−m, indicating that the area of MRNFs and the distance of the MRNFs to the macula affect patients’ visual prognosis. This explains why, in some cases, although aggressive treatments were applied, many patients did not respond well to treatment.[1] These results suggest that doctors should set realistic expectations among patients for the final recovery of vision.
In addition to the new insights into the associations between MRNFs and CDVA, our study also investigated the correlations between MRNFs and △SER, SER, and AL. In the present study, the area and location of MRNFs were also correlated with patients’ SER, AL, and △SER. The larger the area of the MRNFs, the worse the SE, AL, and △SER. Regarding △SER, in contrast to our findings, Kee et al.[14] found no statistical correlation between the extent of myelination and the amount of anisometropia. The underlying reason contributing to these discrepancies may be that we used ultra-wide-field images to calculate the full area of MRNFs, while Kee et al. used clock hours of retinal involvement. Clarus is an ultra-wide-field fundus camera that obtains approximately 133° in a single capture and 220° in a montage mode, which makes it possible to obtain a full view of MRNFs in comparison with traditional fundus cameras.
The area of MRNFs was also found to be associated with patients’ ReT_VS and ChT_VS, but not with foveal ReT, ChT, ReT_VI, or ChT_VI. The underlying reason may be that MRNFs were more often distributed at the superior and inferotemporal areas of the optic disc rather than other areas. Consistent with our results, Straatsma et al.[5] reported a similar result of MRNF distribution in 42 patients with MRNFs. The MRNF-involved retina tends to be thicker,[12] which results in compression of the choroid and causes a reduction in choroid thickness.
Knowledge of the microvascular metrics of the retina and choroid can help differentiate it from other intraretinal lesions or elucidate the mechanism underlying the association of axial myopia with MRNFs. Previous studies reported that there was no significant difference in FAZ between the myopia and the non-myopia groups in patients without MRNFs.[15, 16] In the present study, we did not find any statistical difference in FAZ parameters, including FAZ, FAZP, FAZ-CI, and FD-300, between the eyes with and without MRNFs. However, we did not evaluate microvessel density metrics other than FAZ parameters because thick MRNFs could result in intense posterior shadowing with loss of structural and vascular information of the retina and choroid.
As for choroidal thickness, the foveal ChT, ChT_VI, and ChT_VS were significantly thinner in the affected eyes. Two reasons may have contributed to this finding. First, the thickened MRNF-involved retina compressed the choroid, resulting in a decrease in choroid thickness. Second, affected eyes tend to show axial high myopia, and the progression of myopia has been suggested to be associated with elongation of the eyeball, mechanically stretching the retina and causing a reduction in the retinal nerve fiber layer thickness, retinal microvascular density, and choroid thickness.[15, 17] Consistent with these findings, the SER and AL were closely correlated with ChT in the unaffected eyes in our study (mean SER: -3.90 ± 3.94 D; range, -13.25 to 0.75 D).(Table 3) Therefore, to distinguish the factor causing thinning of the choroid, the ideal study design would include other age-, sex-, and SER-matched controls. However, age- and sex-matched children with super-high myopia are rare in clinics, making them very difficult to recruit. Thus, further studies with better designs are necessary.
This study had two limitations. First, the sample size was small, which may have limited the precision of the results. However, the prevalence of patients with MRNFs is very low; therefore, it is difficult to include a large number of patients. Second, MRNFs could be isolated, or associated with myopia, anisometropia, amblyopia syndrome, optic nerve diseases,[18, 19] and systemic diseases.1 None of the patients in the present study had systemic diseases, so the findings of the present study could not be extrapolated to other situations.
In summary, the findings of the present study suggest that the presence of MRNFs impacts CDVA and ReT at the fovea, especially ReT_VS. The area of MRNFs, as well as the distance from the MRNFs to the fovea, are closely associated with the affected eyes’ CDVA, SER, AL, the amount of anisometropia, ReT_VS, and ChT_VS. These findings could help doctors judge the visual prognosis of patients and elucidate the mechanism underlying axial myopia associated with MRNFs in the future.
{kind=link}