This study offers vital insights into the intricate relationships that older persons in India have between indoor air pollution, health, and life happiness. The significant direct negative association between indoor air pollution and life satisfaction, coupled with the mediation effect of health, highlights the multifaceted impact of environmental factors on elderly well-being.
Our research found that the detrimental effects of indoor air pollution on life satisfaction are in line with general worldwide trends. For instance, studies across various countries have demonstrated similar detrimental effects of poor air quality on health and psychological well-being (Ezzati & Kammen, 2002; Pope III, 2002). The health burden from indoor air pollution is significant in areas like Sub-Saharan Africa and Southeast Asia, where biomass fuel use is common. These conditions frequently result in severe respiratory and cardiovascular disorders, which have a direct negative impact on life quality and longevity (Bonjour et al., 2013; Lim et al., 2012). Moreover, research from developed countries provides a contrast, showing that improvements in air quality can lead to significant enhancements in population health and well-being. For example, interventions in the United States and Europe that have focused on reducing air pollution levels have been associated with improved life expectancy and reduced disease incidence, which contribute to higher life satisfaction ratings among the affected populations (Smith & Sagar, 2014).
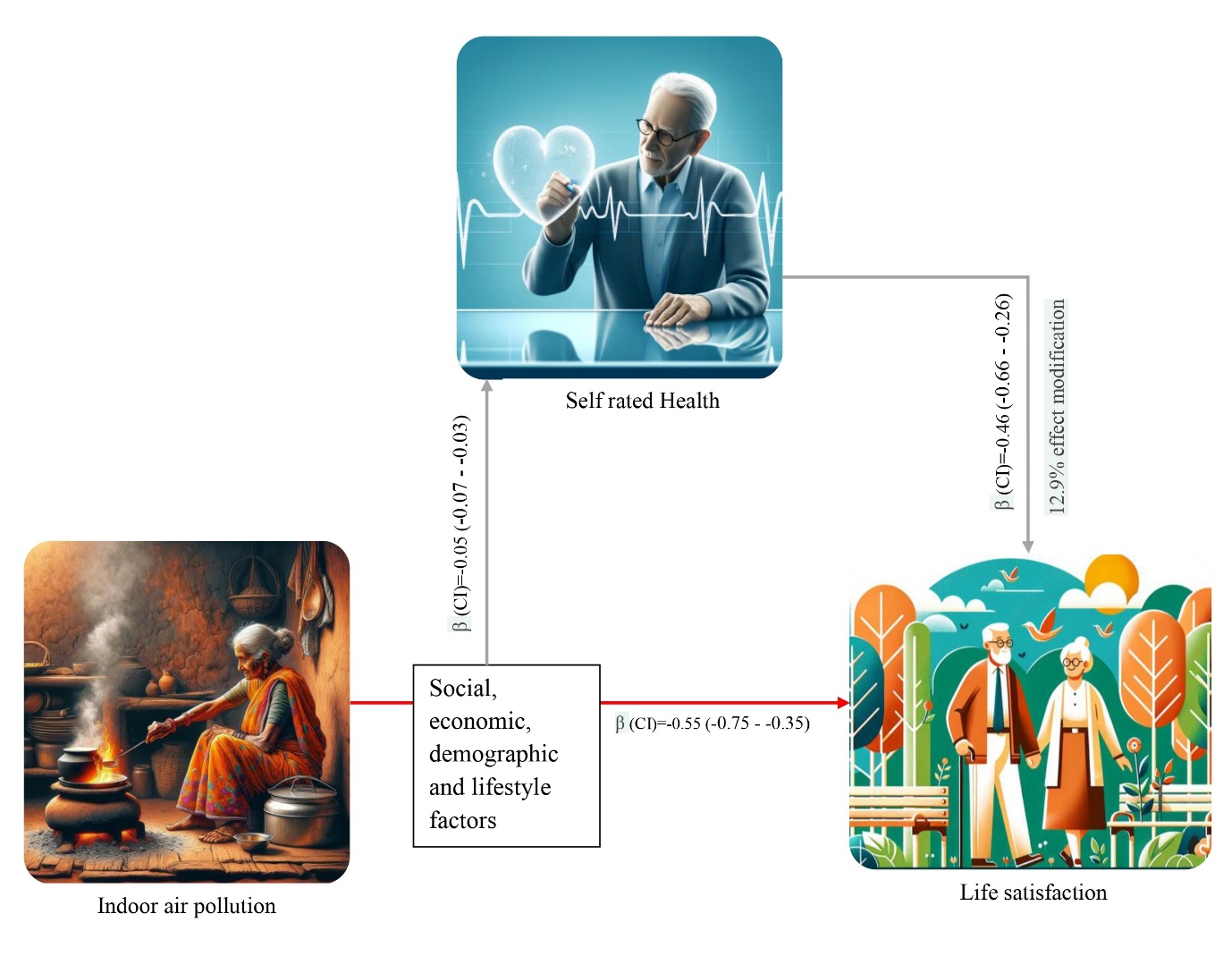
In the context of our study, health significantly mediates the impact of indoor air pollution on life satisfaction among older adults. This mediation underscores the complexity of how physical health conditions, exacerbated by environmental pollutants, directly contribute to the subjective perception of quality of life. Health mediation suggests that the effects of indoor air pollution on life satisfaction are not completely direct but are filtered through the changes in health status that pollution induces. Particulate matter and hazardous compounds derived from biomass fuels are examples of pollutants that can cause respiratory issues, cardiovascular disorders, and long-term ailments, including bronchitis and asthma (Lim et al., 2012; Smith & Sagar, 2014). These health issues can severely limit daily activities, increase medical costs, and induce stress and anxiety, which cumulatively decrease life satisfaction.
The linkage between indoor air pollution and socio-economic status is critical. In India, lower socio-economic groups are more likely to use traditional cooking fuels due to their lower cost and accessibility despite the higher health risks associated (Smith & Sagar, 2014). This leads to a vicious cycle in which low health outcomes are both a cause and an effect of poverty, deepening inequalities and lowering life satisfaction in these areas (Hajat et al., 2014). These socio-economic dimensions are crucial for understanding the barriers to adopting cleaner technologies and fuels. Cultural preferences, lack of awareness, and inadequate infrastructure also play significant roles in perpetuating reliance on traditional fuels, suggesting that policy interventions must be multifaceted and culturally sensitive to be effective (Dabadge et al., 2018).
Our findings underscore the need for integrated public health policies that address both the environmental and social determinants of health. First, there is a clear need for policies that facilitate the transition to cleaner cooking fuels through subsidies, incentives, and infrastructure development. Programs like the Pradhan Mantri Ujjwala Yojana have made strides but must be expanded and combined with educational campaigns that emphasize the health benefits of reduced indoor air pollution (The Hindu, 2018). Second, healthcare interventions should focus on screening, early detection, and treatment of pollution-related health issues among older adults. Establishing community health programs that monitor symptoms and provide treatment at local levels can help mitigate the health impacts more effectively. Third, urban planning and housing regulations should incorporate guidelines to improve indoor air quality. This includes better ventilation systems, the use of non-toxic building materials, and green spaces in urban areas, which have been shown to improve overall air quality and enhance life satisfaction (Lim et al., 2012; Prüss-Üstün et al., 2016).
While our study provides insightful findings, it is not without limitations. The cross-sectional design restricts our ability to infer causality between indoor air pollution, health, and life satisfaction. A more conclusive knowledge of these correlations may be obtained through longitudinal investigations. Additionally, the reliance on self-reported measures for health and life satisfaction may introduce bias, highlighting the need for objective health indicators in future research.
Further research should explore longitudinal data to establish causal relationships and assess the long-term impacts of air quality improvements on health and life satisfaction. Additionally, studying other potential mediators like mental health, social support, and access to health services could provide a deeper understanding of the pathways through which environmental conditions influence life satisfaction. Comparative studies across different cultural and economic settings would also be valuable in generalizing the findings and tailoring interventions accordingly (Hajat et al., 2014).
{kind=link}