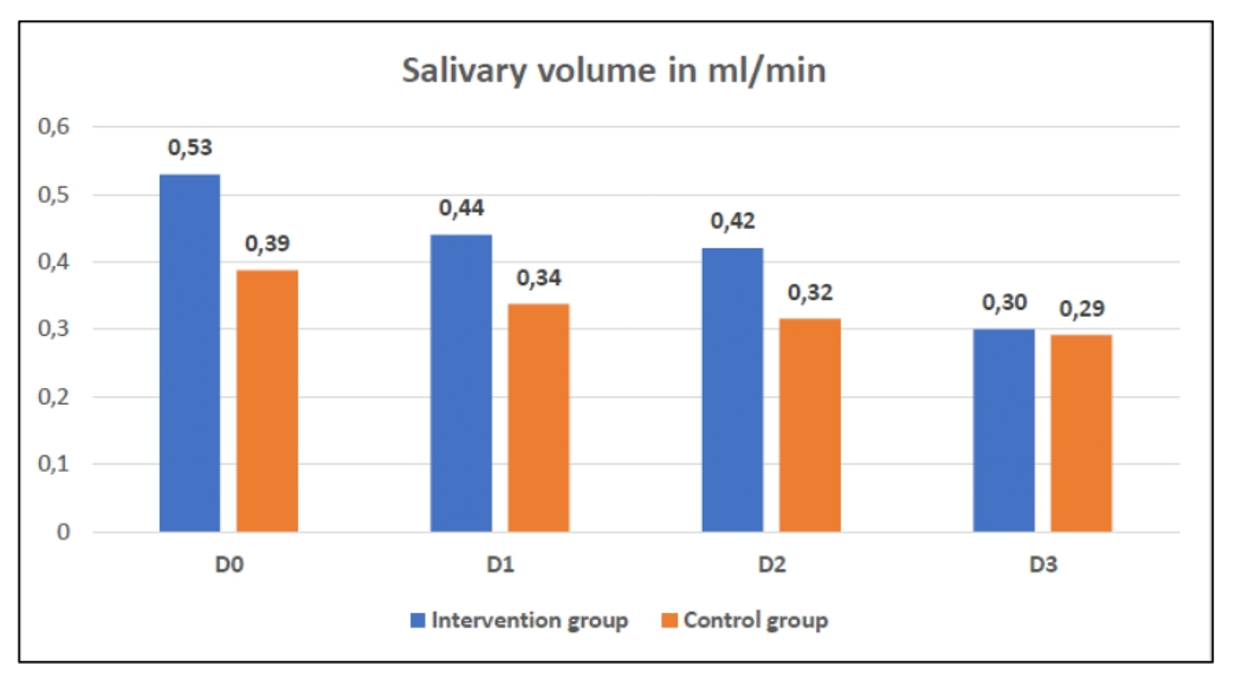
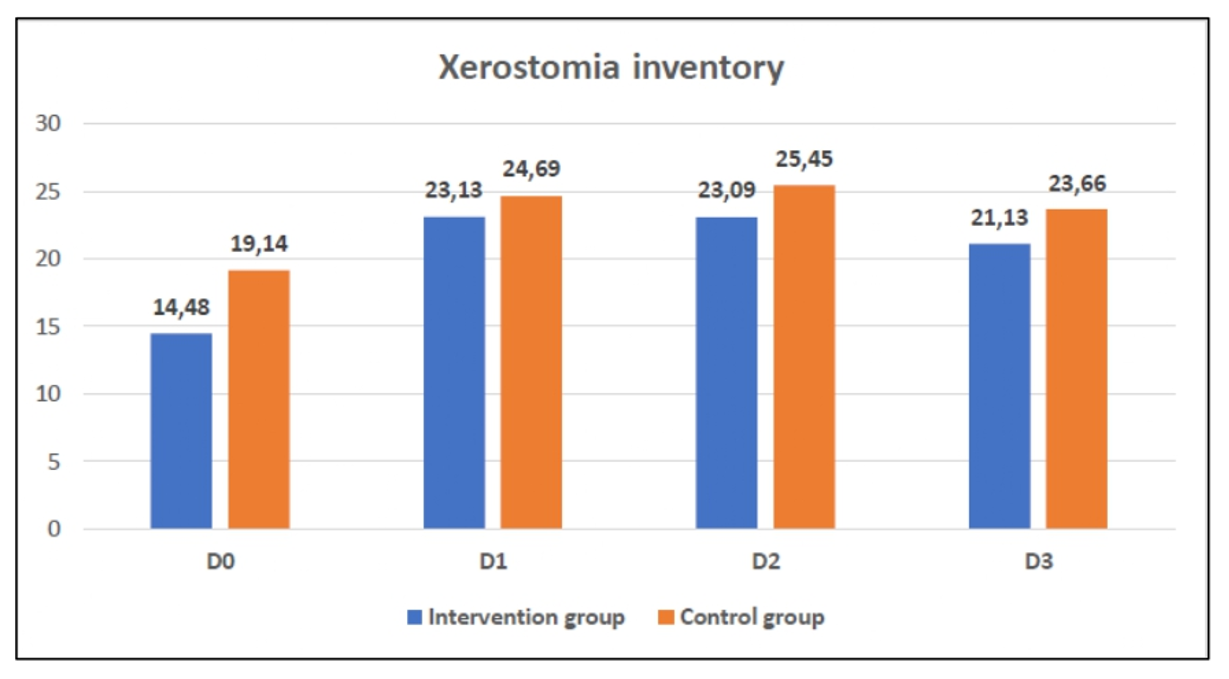
To date, few data are available on the effectiveness of extra-oral PBM in preventing xerostomia/hyposalivation in patients undergoing cancer treatment. A recent randomized clinical trial showed that photobiomodulation contributed to the improvement of xerostomia and OM, preventing patients from progressing to higher degrees of xerostomia and preventing and treating OM lesions [31]. A study evaluating the role of PBM in preventing xerostomia demonstrated that PBM used to treat OM can be effective in alleviating the symptoms of RT-induced xerostomia [32]. Another study suggested that the use of PBM did not prevent the reduction in salivary flow associated with TR but appeared to prevent patients from progressing to higher degrees when measuring salivary flow [3]. The results of the present study showed that the two protocols used with infrared laser were able to keep patients with RSF within normal parameters during and after RT, but extraoral stimulation of the salivary glands was associated with a lower prevalence and severity of xerostomia in patients who received the intervention compared to the placebo group. The fact that the control group also did not progress to hyposalivation leads us to believe that even PBM performed with the aim of preventing OM seems to positively influence the stimulation of the salivary glands, even if the benefits are discrete.
It was observed that patients who did not have their salivary glands stimulated through extraoral PBM presented, in addition to a higher prevalence of xerostomia, more associated complications such as dysphagia, oral pain, OM, and fungal infection, which are the most common complications in the sample. This goes against what has been described in the literature, which is the most frequent complication of OM, xerostomia, dysgeusia, dysphagia, trismus, dermatitis, and candidiasis [33]. These complications influence the appetite and intake of patients, which can lead to inadequate levels of energy and nutrients, causing malnutrition. A randomized clinical trial of patients undergoing head and neck radiotherapy showed that xerostomia was the most important factor associated with weight loss in cancer survivors after completion of RT. Malnutrition can lead to interruption in treatment with impaired prognosis as well as a negative impact on the QoL of these patients [34]. The findings of this study demonstrated that no patient had to interrupt treatment for oral complications.
When considering the causes that contribute to the development of xerostomia and/or hyposalivation, damage to the parotid and submandibular glands is considered to be the main salivary gland that produces more than 80% of saliva [35]. Greater damage to the salivary glands was expected in the intervention group since most patients had the oropharynx region as a tumor location, making it more difficult to preserve part of the larger salivary glands from radiation. This expectation was not confirmed, with a greater reduction in flow in the control group, in which the most frequent location was the larynx. This could be explained by the fact that most tumors have advanced staging, thus requiring broader irradiation fields. When possible, reducing the dose to parotids leads to the preservation of salivary function after RT. In this study, the most frequent locations were the oropharynx and larynx, similar to what has been previously described in the literature. In a study that evaluated the dosimetry of LLLT for OM, 363 patients with head and neck cancer and the most frequent location were evaluated as the oral cavity, followed by the oropharynx and larynx [36].
The literature highlights that the occurrence of hyposalivation is related to several factors, such as the radiation dose, volume of irradiated tissue, and use of concomitant CT for radiation sensitization [37]. In this study, there was a greater presence of CT concomitant with RT in the control group, which also showed lower values of salivary flow throughout the treatment when compared with the group subjected to extraoral PBM. However, no data are available in the literature to confirm this relationship. In an antagonistic way, studies show that the addition of CT administered concomitantly with RT was not responsible for a greater severity of xerostomia when compared to RT alone, unlike complications such as OM, which presents a greater risk of occurrence when the two treatments are combined [38, 39]. As for the relationship between the RT dose and salivary gland dysfunction, all patients in the sample were exposed to a dose susceptible to irreversible damage, since the doses varied between 50 Gy and 70 Gy, with the average dose being higher in the intervention group. Literature demonstrates that damage to the salivary glands becomes irreversible after cumulative doses greater than 50 Gy [16]. As the entire sample was exposed to sufficiently high doses, it was not possible to establish comparative parameters between the groups.
The standard treatment for RT for head and neck squamous cell carcinoma changed from 2D RT to 3D RT and later to intensity-modulated RT (IMRT) [40]. In the samples studied, treatment with 3D RT predominated, followed by 2D RT. No patient underwent IMRT because this technology was not available in the hospital where the study was conducted. The limitation presented favors the results found because if it were possible to keep patients without low salivary flow during 3D RT, it is believed that with a more modern technique that preserves greater glandular volume, the results would be even better. Clinical research proving the benefits of lasers in preventing and/or treating low salivary flow remains scarce. A narrative review and meta-analysis showed that studies found that extraoral stimulation of the salivary glands brings benefits in hyposalivation and changes in salivary flow resulting from RT injuries [41]. In contrast, a pilot study that evaluated the effect of LLLT on xerostomia and hyposalivation caused by RT reported that in the parameters used, PBM was not able to increase PBM or decrease xerostomia, and associated these negative results with the late effects of RT on the glandular structure, such as fibrosis and acinar atrophy [42]. A scoping review showed that prophylactic physical salivary stimulation therapies can produce better effects than therapeutic applications [43]. This finding, in addition to the results presented in this research, highlights the possible benefit of stimulating the salivary glands concomitantly with TR or TR + CT. It should be noted that the effects of PBM are transient and there is no consensus in the literature on the duration of the desired effect. Therefore, studies with longer follow-ups must be conducted so that it is possible to observe the maintenance of the desired effect, providing long-term benefits.
{kind=link}
{kind=link}