The study used a two-sample MR method to explore the causal relationship between CKD and cognitive dysfunction. The MR results showed that this causal connection existed. Furthermore, we also discovered a link between CKD and cognitive dysfunction via the gut microbiome using a two-step MR study. Encouragingly, we found that some gut microbiota could mediate or moderate this relationship.
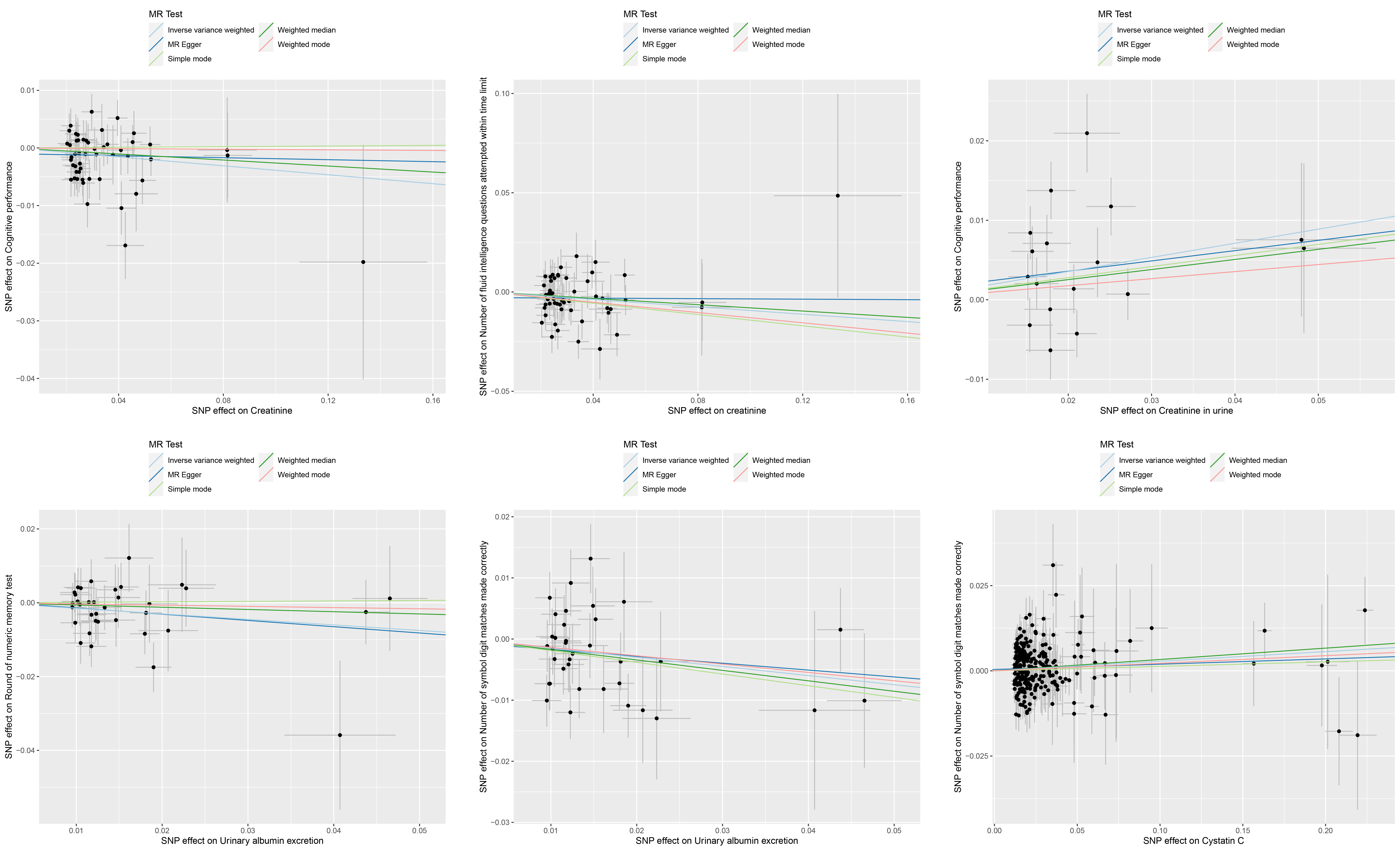
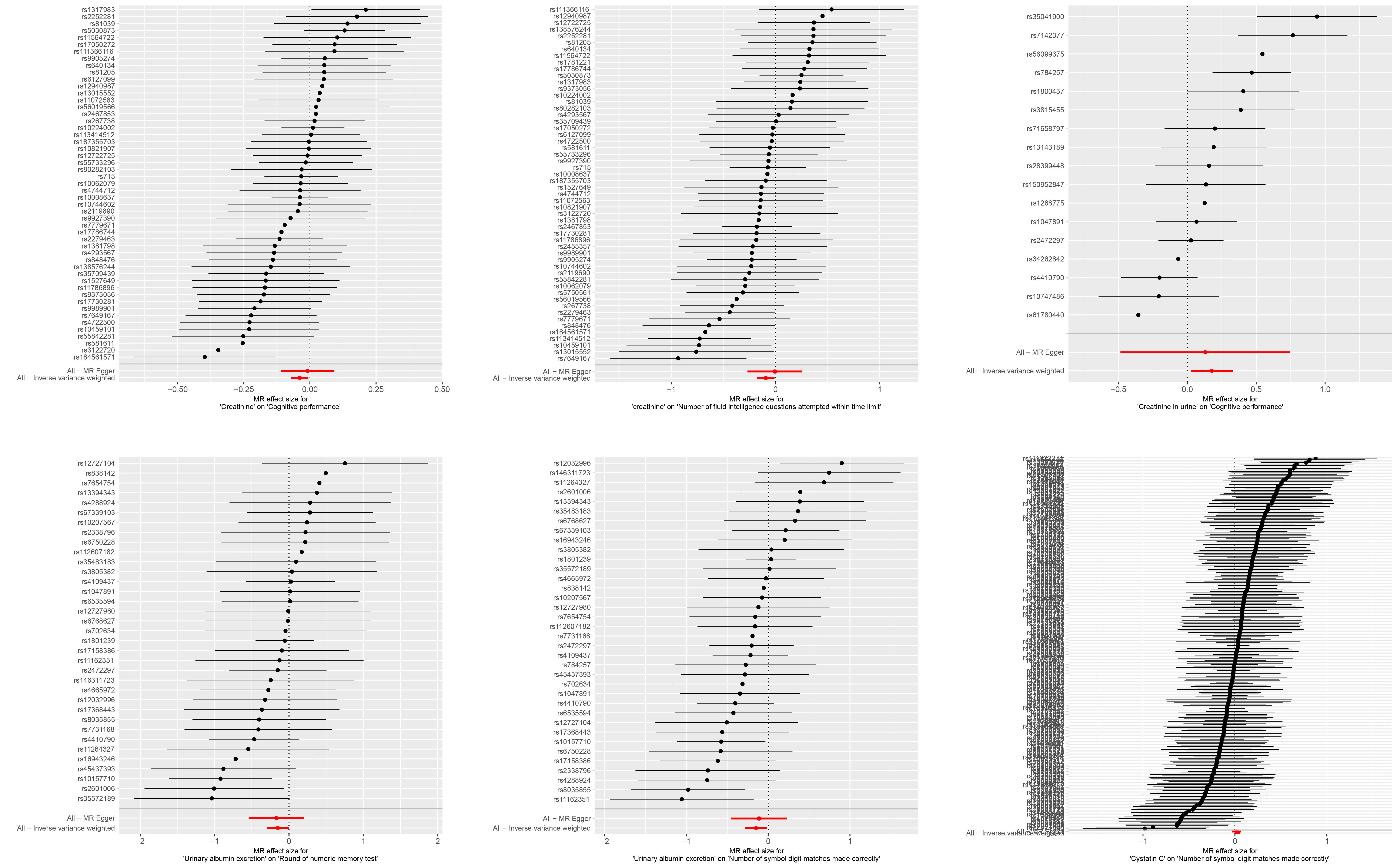
The two-sample MR analysis revealed intriguing associations between renal biomarkers and cognitive performance. In some ways, the current study is similar to earlier research, but not completely. Previous studies have mixed results, with most comparing cognitive outcomes based on eGFR[36–39]. Due to discrepancies in the directional estimations of the link between GFR and cognitive function, GFR was excluded from our primary outcome presentation. Studies involving kidney damage markers (i.e., albuminuria or proteinuria) have been more consistent in reporting cognitive function associations[36, 40, 41]. This is in line with our observations that urinary albumin excretion demonstrated an inverse relationship with cognitive performance, indicating that albuminuria could be a potential risk factor for cognitive impairment. Furthermore, our study contributes to the emerging evidence that serum cystatin C may be a risk factor for cognitive decline. This finding is consistent with the hypothesis that inflammation and vascular damage, which are often associated with kidney disease, can have detrimental effects on cognitive function[42, 43]. Conversely, the observation that high creatinine levels may improve memory and learning functions challenges conventional understanding[44]. Our study suggests a potential protective role of creatinine in cognitive processes, as indicated by the ORs for fluid intelligence questions and overall cognitive performance. The unexpected positive association between urinary creatinine levels and cognitive performance introduces a layer of complexity. This warrants further investigation, as it could indicate a more complex interplay between renal function markers and cognitive health than previously recognized. This divergence may reflect distinct metabolic pathways or the influence of other, as yet undefined, factors.
The exploration of the GM mediating role in the causal pathway from CKD to cognitive dysfunction represents a significant advancement in our understanding of the complex interplay between renal health and cognitive function. Building upon previous research that implicated creatinine levels and alterations in the GM, our study introduces a two-step MR approach. This methodological choice allowed us to rigorously investigate the potential mediating effects of the GM in a manner that leverages the strengths of genetic instrumental variables to infer causality.
Creatinine, a metabolic waste product, accumulates in the blood as kidney function declines[45]. Healthy kidneys easily remove creatinine from the circulation via urine; however, impaired kidney function can result in lower creatinine excretion in the urine[46]. The elevated levels of creatinine in the blood can lead to protein loss[45, 48]. This protein loss could alter the gut environment, potentially favoring the growth of certain microbial species over others and leading to dysbiosis[16, 17, 45, 47]. Our findings, which demonstrate a significant association between creatinine levels and various gut microbiota taxa, support the hypothesis that renal function has a direct influence on the gut microbiota.
Our MR analysis's second step uncovered a link between gut microbiota and cognitive function, with specific taxa exerting both positive and negative impacts on cognitive performance. In humans, the predominant Archaea are methanogens in the gastrointestinal system, which may mitigate ROS and trimethylamine N-oxide (TMAO) production as well as intestinal permeability[48]. It is established that patients with CKD exhibit dysbiosis and an increased production of uremic toxins, including TMAO, which contribute to oxidative stress and inflammation[49]. Methane, produced by these methanogens, could play an indirect role in mechanisms that regulate the antioxidant response[48]. Despite this, some studies offer divergent results. Relative to healthy individuals, methanogens are disproportionately present in patients with conditions such as inflammatory bowel disease[50], periodontal disease[51], obesity, cancer[52], and diverticulosis[52]. Furthermore, methanogens have been recognized for their capacity to activate dendritic cells from human monocytes, which can lead to potent inflammatory responses[53]. In recent years, a connection between methanogens and neurological disorders, notably multiple sclerosis (MS), has been noted[48, 54]. Our research has revealed an intriguing finding: the class Methanobacteria, the order Methanobacteriales, and the family Methanobacteriaceae may have a negative impact on cognitive ability. However, research into the role of methanogens in inflammation and chronic diseases remains in its early stages, with the precise mechanisms of their impact on human health yet to be fully understood.
The Eubacterium fissicatena group is renowned for its species that metabolize butyrate, a short-chain fatty acid (SCFA) derived from dietary carbohydrates[55]. Butyrate plays a pivotal role in the colonic inflammatory response and possesses anti-inflammatory characteristics. It is also crucial for maintaining the integrity of tight junctions, thereby preventing dysbiosis and gut permeability issues[56, 57]. A protective association has been genetically predicted between the abundance of the Eubacterium fissicatena group and Alzheimer's disease (AD)[58]. Consistent with previous findings, we found that the Eubacterium fissicatena group's negative correlation with the number of fluid intelligence questions attempted within the time limit suggests its potential to detract from cognitive function. These findings support the emerging perspective that the gut microbiota is a modifiable factor that could significantly influence cognitive health. The identification of specific classes and genera that exhibit significant mediation effects provides preliminary evidence for a modifiable pathway that could be targeted in interventions aimed at improving cognitive outcomes in individuals with CKD.
Our study's strengths lie in its innovative use of a two-step MR approach and the comprehensive evaluation of a wide range of renal and cognitive biomarkers. The study leverages MR analysis, offering distinct advantages in the investigation of causality. As a novel genetic statistical approach, MR provides a robust framework for discerning causal relationships by utilizing genetic variants as IVs. This method circumvents many of the challenges associated with traditional observational studies, such as confounding factors and the issue of reverse causality.
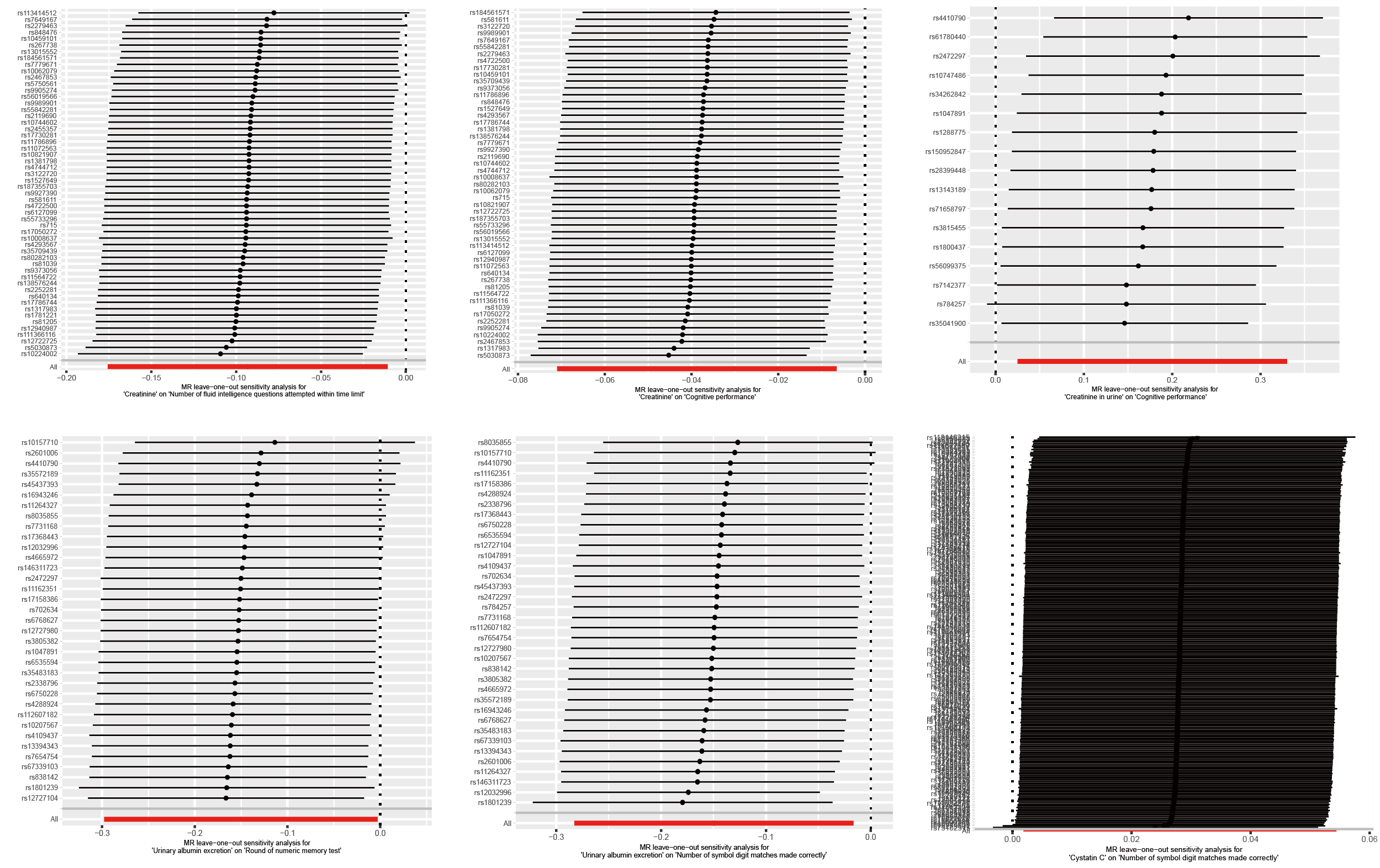
However, our study has several limitations. Firstly, the generalizability of our findings is limited by the fact that the genetic data from GWAS were derived exclusively from individuals of European ancestry, which restricts the applicability of our conclusions to other racial and ethnic groups. Secondly, the potential for significant overlap in SNP data across various taxonomic ranks, such as phylum, class, order, family, and genus, may affect the reproducibility of the MR analysis results. There is the potential for residual confounding due to the exclusion of certain taxa and the reliance on urinary creatinine as a proxy for renal function. This overlap could introduce bias or reduce the precision of the estimated causal effects. Lastly, the limitations of GWAS meta-analysis data prevent the investigation of stratification effects and nonlinear associations between CKD and gut microbiota risk. The assumption of linearity may not capture the complexity of biological processes. Future research incorporating more granular GM classification and diverse ancestry data is warranted to address these limitations and further validate the observed associations. Despite these possible limitations, we have demonstrated through a variety of sensitivity studies that the causal estimates in this study were robust.
{kind=link}
{kind=link}
{kind=link}