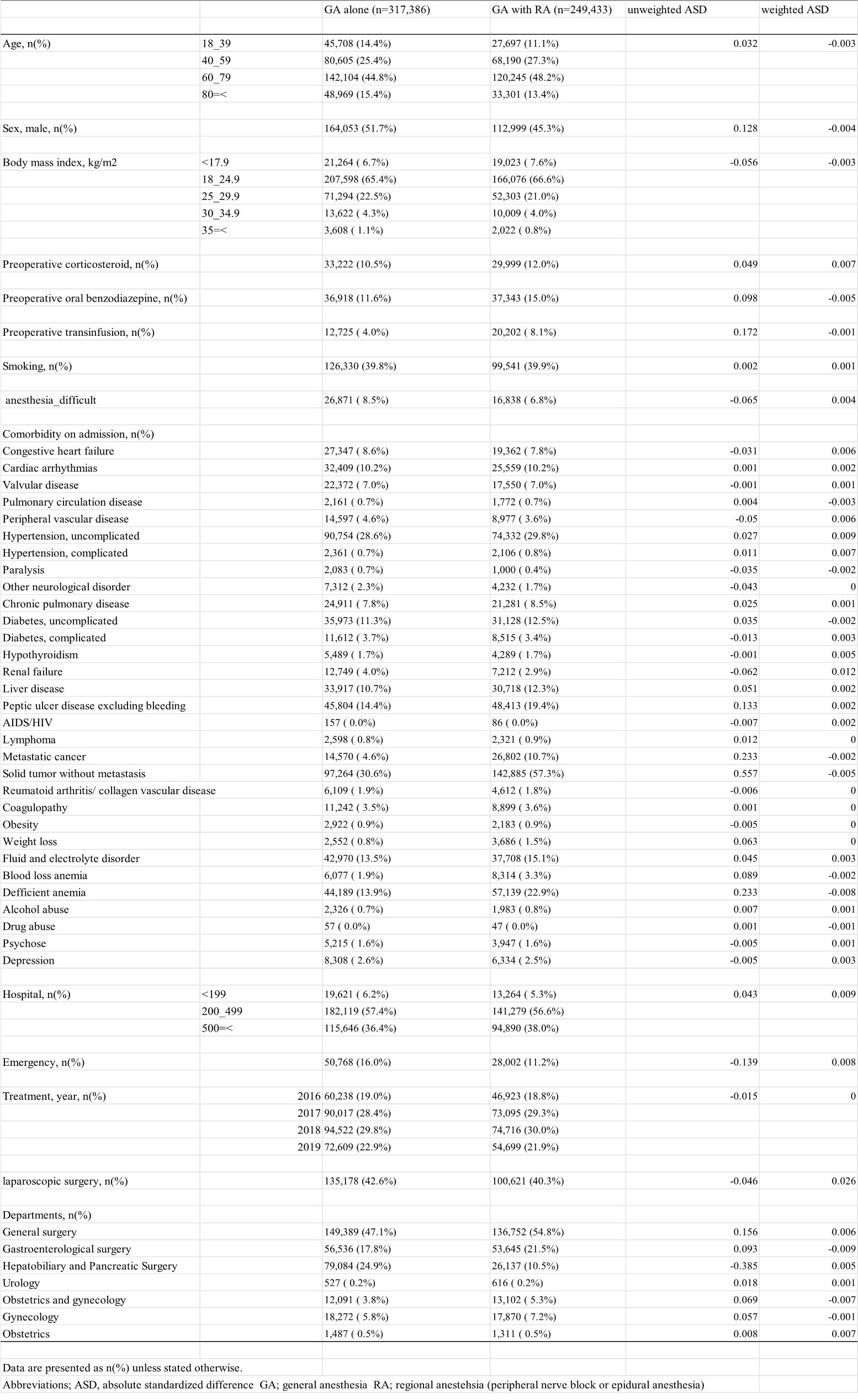
We selected 698,078 patients who had undergone abdominal surgery during the study period. We then excluded 2,427 patients in whom the anesthesia duration was more than 1,440 min, 69,475 patients who underwent multiple surgical procedures per admission, 45,791 patients who were not extubated, and 13,566 patients who had missing values. A total of 566,819 patients who met the inclusion criteria were divided into the GA–RA group (n=249,433) and the GA-alone group (n=317,386) (Figure 1). Overall, 148,105 patients (59.4%) in the GA–RA group and 132,819 (41.8%) in the GA-alone group experienced PONV. Table 1 shows the baseline characteristics of the patients in each group. No significant differences in the baseline characteristics were noted between the groups after sIPTW (c-statistic: 0.72).
Figure 2 shows the results of the sIPTW Kaplan–Meier analysis. Overall, after sIPTW, the incidence of PONV was 57.2% in the GA–RA group and 47.1% in the GA-alone group.
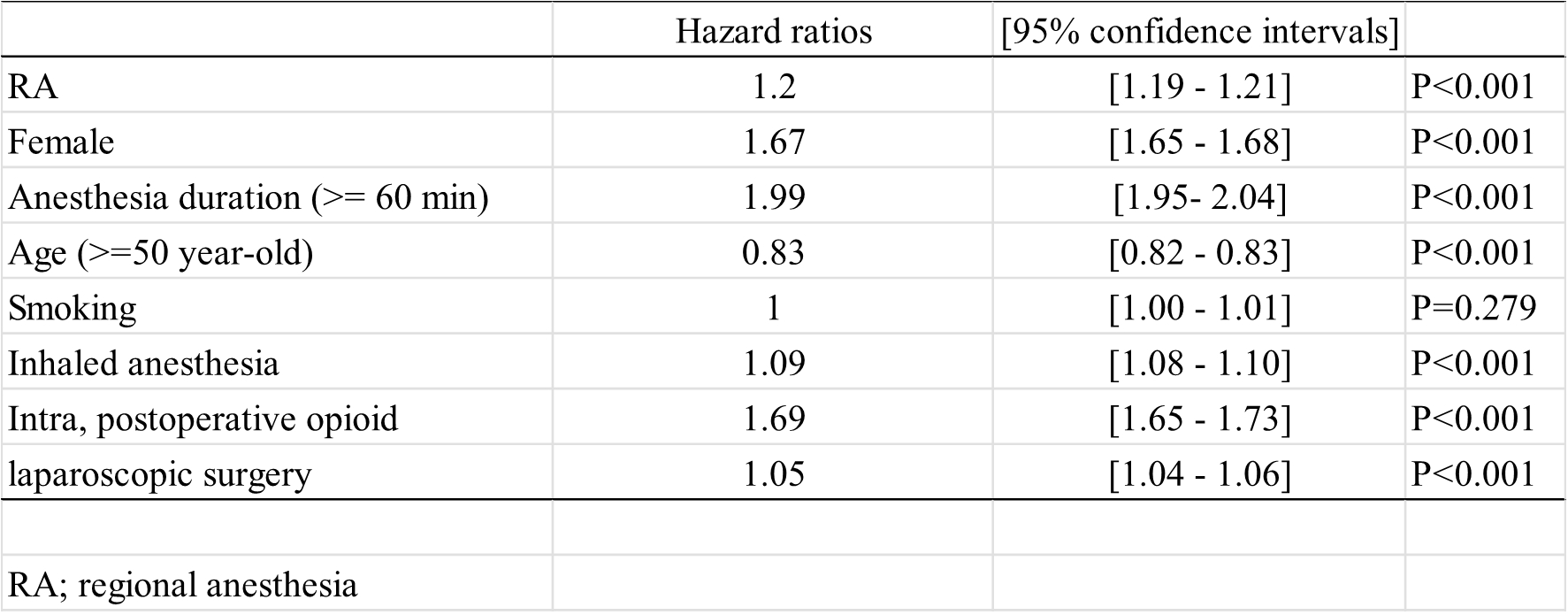
The sIPTW univariable Cox regression analysis revealed a slight difference in the overall incidence of PONV (HR, 1.25; 95% CI, 1.24 to 1.26; P<0.001) between the GA–RA and GA-alone groups. Table 2 shows the HRs for PONV incidence that were determined using the sIPTW multivariable Cox regression analysis. Patients were higher odds RA (HR, 1.20; 95% CI, 1.19 to 1.21; P<0.001), female sex (HR, 1.67; 95% CI, 1.65 to 1.68; P<0.001), inhaled anesthesia (HR, 1.09; 95% CI, 1.08 to 1.10; P<0.001), intraoperative or postoperative opioid usage (HR, 1.69; 95% CI, 1.65 to 1.73; P<0.001), laparoscopic surgery (HR, 1.05; 95% CI, 1.04 to 1.06; P<0.001), and lower age (HR, 0.83; 95% CI, 0.82 to 0.83; P<0.001). Proportional hazards are presented in Supplementary figure 1 and 2.
The E-value indicated that a confounder would have to be associated with the exposure and PONV by a value of 1.53 each on a relative risk scale to negate the observed association between GA with RA and PONV. Similarly, the CI for the observed association with PONV could be moved to include the null by an unmeasured confounder associated with exposure and PONV by a factor of 1.51.
The results of the subgroup analyses are presented in figure 3. The sIPTW multivariable Cox regression analysis revealed a slight difference in the overall PONV incidence (HR, 1.15; 95% CI, 1.14 to 1.16; P<0.001) between the GA–PNB (n=54,792) and GA-alone groups. The analysis also revealed a difference in the overall PONV incidence (HR, 1.24; 95% CI, 1.23 to 1.25; P<0.001) between the GA–EA (n=194,641) and GA-alone groups. GA–PNB and GA–EA were associated with PONV incidence after abdominal surgery.
The sIPTW RMST analysis revealed an RSMT of 1.05 (95% CI, 1.05 to 1.06) days in the GA–RA group and 1.27 (95% CI, 1.26 to 1.27) days in the GA-alone group. The difference in the mean survival time was 0.21 days (95% CI, 0.21 to 0.22; P<0.001). This indicates that the PONV incidence was higher in the GA–RA group near the date of surgery.
{kind=link}
{kind=link}