At present, the therapeutic effect and maintenance time of LipiFlow are relatively clear, however, there are few studies on the efficacy of MiBoFlo. The purpose of this study is to explore the short-term therapeutic effects of MiBoFlo on MGD patients in China.
The OSDI score observed in both groups improved significantly at the first visit. There was no significant change in 2-month follow-up, however, compared with baseline level, the changes were still clinically meaningful.
A study published by Kimberly L recruited 310 subjects in order to assess the minimal clinically important difference(MCID) for the OSDI, which is defined as “the smallest difference in score in that domain of interest which subjects perceive as beneficial and which would mandate, in the absence of troublesome side effects and excessive cost, a change in the patient’s management.”16 It found that the MCID ranged from 4.5 to 7.3 for mild or moderate disease and from 7.3 to 13.4 for severe disease,17 and it suggested that the response to treatment among patients with severe symptoms should be set higher than the response to treatment among patients with moderate symptoms. Thus, in our study, by calculating the difference of OSDI score between baseline and 2-month follow-up for each patient, we found that in MiBoFlo group, the mean improvement for severe patients was 11.3, and for mild to moderate patients was 5.5, and in LipiFlow group, the mean improvement for severe patients was 10.7, and for mild to moderate patients was 5.1, which indicated that both devices were meaningful for the improvement of DED patients’ unpleasant symptoms.
It is a remarkable fact that due to the feature of the separation of dry eye symptoms and signs,18 the patient’s “severe” OSDI score cannot indicate that he/she is a patient with severe dry eye. The severity of DED is to be comprehensively evaluated with symptoms and signs.
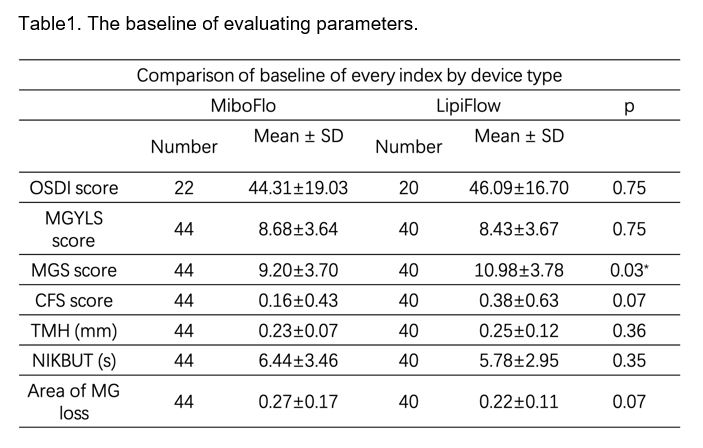
Based on the pathogenesis, observing the orifice and meibum is the easiest and most direct way for objective signs evaluation. Thus, MGYLS and MGS were chosen as main outcome parameters for meibomian gland assessment. From this study, we can see that the MGYLS and MGS observed in MiBoFlo group improved significantly in both 1-month and 2-month follow-up visit. It was worth noting that the results of LipiFlow group revealed a more obviously trend of continued improvement in 1-month follow-up period.
From the comparison of two groups, the LipiFlow treatment was more like a “one-step process”, and the MiBoFlo treatment seemed to be “layer by layer”. For the difference of treatment effects between two groups, there could be following reasons through analysis. First of all, although both MiBoFlo and LipiFlow achieve the therapeutic effect by transferring heat from the device to the meibomian glands, the difference is the actual temperature reaching the meibomian glands. MiBoFlo is an external eyelid-warming device, heat must pass through the eyelid tissue to reach the meibomian glands. Overheating is not advisable in order to ensure security of the skin and cornea. Thus, heat loss is inevitable. LipiFlow is an internal eyelid-warming device and a lid warmer designed to rest on the sclera to transfer heat directly to the palpebral conjunctiva. A research reported by Kenrick CJ showed that the upper palpebral conjunctival temperatures had increased from 37.0℃ to 42.0℃ after 12 minutes LipiFlow treatment, however, after 10 minutes MiBoFlo treatment, the temperatures increased minimally.12
Secondly, the pressure applied to meibomian gland is different either. The pressure of a deliberate blink is about 0.3 psi. As for MGD patients, Korb reported that the pressure required for obtaining the nonliquid meibum varied from 5–40 psi, however, with moderate to significant discomfort.19 During LipiFlow treatment, the eyelids were compressed between the bladder and the lid warmer at 6 psi simultaneously combined with the inserted eye cup. In MiBoFlo group, the method of discharging meibum is to artificially gently massage the outer eyelid during treatment and followed by physical force compression and the applying pressure is human controlled.
Summing up the above, we hypothesize that LipiFlow covered and squeezed the lower 2/3 meibomian glands while uniformly heating, and had the ability to empty abnormal meibum at once. And in MiBoFlo group, the result tended to be the superimposed effect of multiple treatments. The clearing of the obstruction might restore individual glands to a more normal state, manifesting improvement of MGYLS and MGS. The smooth discharge of normal meibum is beneficial to the recovery of tear film homeostasis. Enhanced lubrication from improved aqueous retention leaded to epithelial cell regeneration. Thus, following the tear film stability improvement, the other objective signs would get better, such as TMH, NIKBUT and CFS in this study.
In addition, it was showed that CFS score improvement in MiBoFlo group were significantly more obvious than in LipiFlow group in this study. It may be due to the small palpebral fissure in Chinese, which may cause damage to the ocular surface during LipiFlow treatment.
In this study, Image J was used in analyzing area of MG loss in two groups. Like evaluating MGYLS and MGS score, all MGs of the lower eyelid were analyzed, not just the central MGs, because of the wide range of massage. In the final analysis, it is found that there was no statistical difference in both groups before and after treatment. However, in the study of Arjan et al., it was indicated that the meibomian gland structure might increase after LipiFlow treatment relative to untreated controls.20 The discrepancy between the two studies could be related to the follow-up time and evaluation methods.
Throughout the treatment, no subject in either group experienced any device-related adverse events that involved changes in VA, IOP, anterior segment and facial skin. Only one case in the LipiFlow group encountered difficulties in the process of installing the eye cup because of small palpebral fissure.
Such improvements in subjective symptoms and tear film stability following a painless, relaxing and safe therapy, stand in contrast to the most common treatments for DED patients currently in use, for example, pharmacotherapy. Pharmacological approaches require patient adherence to a dosing regimen that typically involves single or multiple daily doses, often for extended periods of time. Considering that the aqueous supplementation would count for little at the treatment efficacy, we allow patients to continue to use the same eye drops as before, but the medication must remain unchanged during the follow-up.
This is our preliminary study, and our report is not without limitations. Firstly, in this study, it was difficult for us to mask patients and operators, so only the observers could be masked in order to avoid bias as much as possible. Secondly, insufficient number of enrolled patients and follow-up time might cause deviations in the results. In the future clinical management on MGD, clinicians might consider adopting multiple-dose MiBoFlo therapy, or combination therapy with LipiFlow.
{kind=link}