In this study, we developed an innovative electrical neurostimulation method to replicate reflective urination control in awake or urethane-anesthetized SCI mice based on the characteristic activities of the bladder detrusor and sphincter during natural reflective voiding. This new electrical neurostimulation approach comprised IPG electrical stimulation targeting the PN to relax EUS and electrical stimulation of the MPG to control bladder contraction. Our results demonstrate that this novel stimulation induced coordinated bladder contraction and sphincter relaxation, leading to successful reflective voiding. Our findings present a potent electrical neurostimulation strategy aimed at treating NLUTD, reconstructing bladder function, and restoring urinary control in sufferer with SCI. Additionally, they serve as a reference for personalized treatment approaches and the application of unidirectional brain-machine interfaces in urinary function recovery.
SCI impairs the transmission of urinary signals from the PMC to the spinal cord, often leading to NLUTD13,20,21. In recent decades, electrical stimulation therapy has become a key treatment for NLUTD due to its reversibility and controllability. It enhances voiding efficiency post-SCI by delivering artificial signals to the nerves. In this study, given the intact anatomical connections between the MPG and bladder detrusor muscle and the PN innervating the EUS post-SCI2,22,23. This raises the question of whether artificial simultaneous stimulation of the MPG and PN could control relaxation of both the bladder detrusor muscle and EUS, thereby achieving artificial control of voiding post-SCI.
Previous studies have shown that electrical stimulation of the MPG triggers bladder contractions. Thus, the primary challenge of this study was to determine how to artificially control the PN to achieve EUS relaxation. Unlike the PN blocking method, which works through efferent blockade16,24, our approach is fundamentally different and more aligned with the physiological control mechanisms. Specifically, we aimed to artificially transmit appropriate signals to the PN to achieve controlled EUS relaxation.
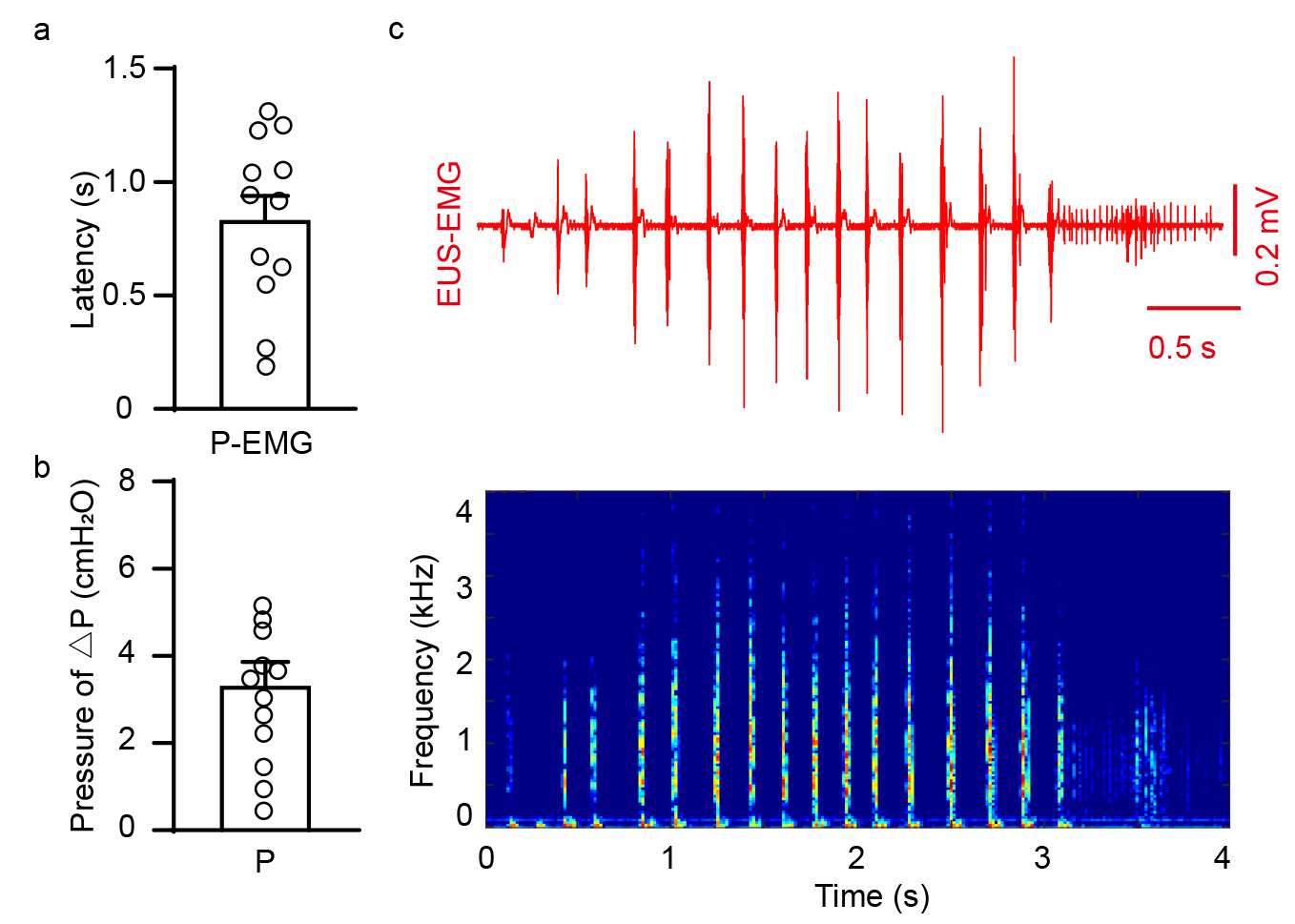
To verify the feasibility of controlling EUS through electrical stimulation, we conducted an in-depth analysis of the normal activity patterns of EUS, extracting key activity characteristics (Fig. 1b-f, Supplementary Fig. 1a-c), and tested them in a mouse model. Although the parameters for achieving artificial control were complex (Table 1), the results were exceedingly exciting. By delivering electrical signals mimicking the activity characteristics of EUS to the PN, we observed an immediate decrease in bladder pressure in a filled bladder and recorded electromyographic (EMG) signals in the EUS that resembled normal physiological activity (Fig. 2a-b, right). This suggests that artificial electrical stimulation might achieve EUS relaxation. To validate the specificity of our simulated electrical stimulation and rule out potential crosstalk during simultaneous electrical recording, we used a single frequency from the simulated information for stimulation. The results showed a continued increase in bladder pressure in the filled bladder, and the simultaneous EUS recordings did not show physiological-like EUS activity (Fig. 2a-b, left).
The potential efficacy of this stimulation pattern may arise from its ability to induce excitatory postsynaptic potentials (EPSPs), leading to a significant recruitment of acetylcholine (ACh) at the synaptic terminals of the PN without causing substantial fatigue to the sphincter25,26. We considered other potential explanations, such as PN stimulation modulating EUS activity through the spinal segmental reflex pathway. Through the activation of pudendal afferents, phasic bursting of EUS increases voiding efficiency27. Le Feber and Van Asselt's study supports this mechanism28. The successful induction of EUS relaxation demonstrates the potential for achieving the key medical objective of protecting the upper urinary tract by maintaining low bladder pressure. In conclusion, these findings indicate that artificial electrical stimulation of the PN can achieve EUS relaxation, presenting a new possibility for the artificial control of EUS and laying the foundation for future artificial coordinated control of voiding and human-machine interaction control.
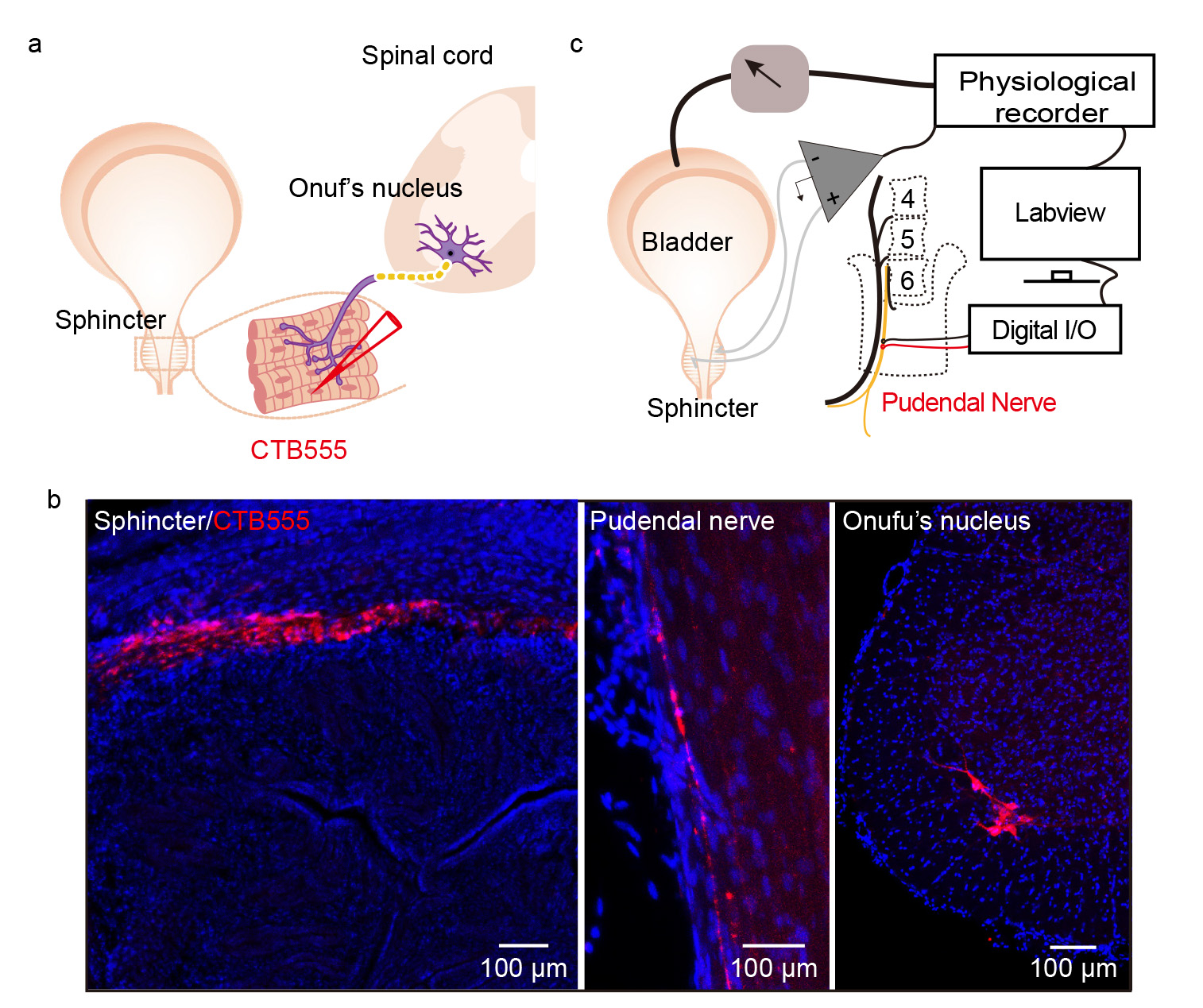
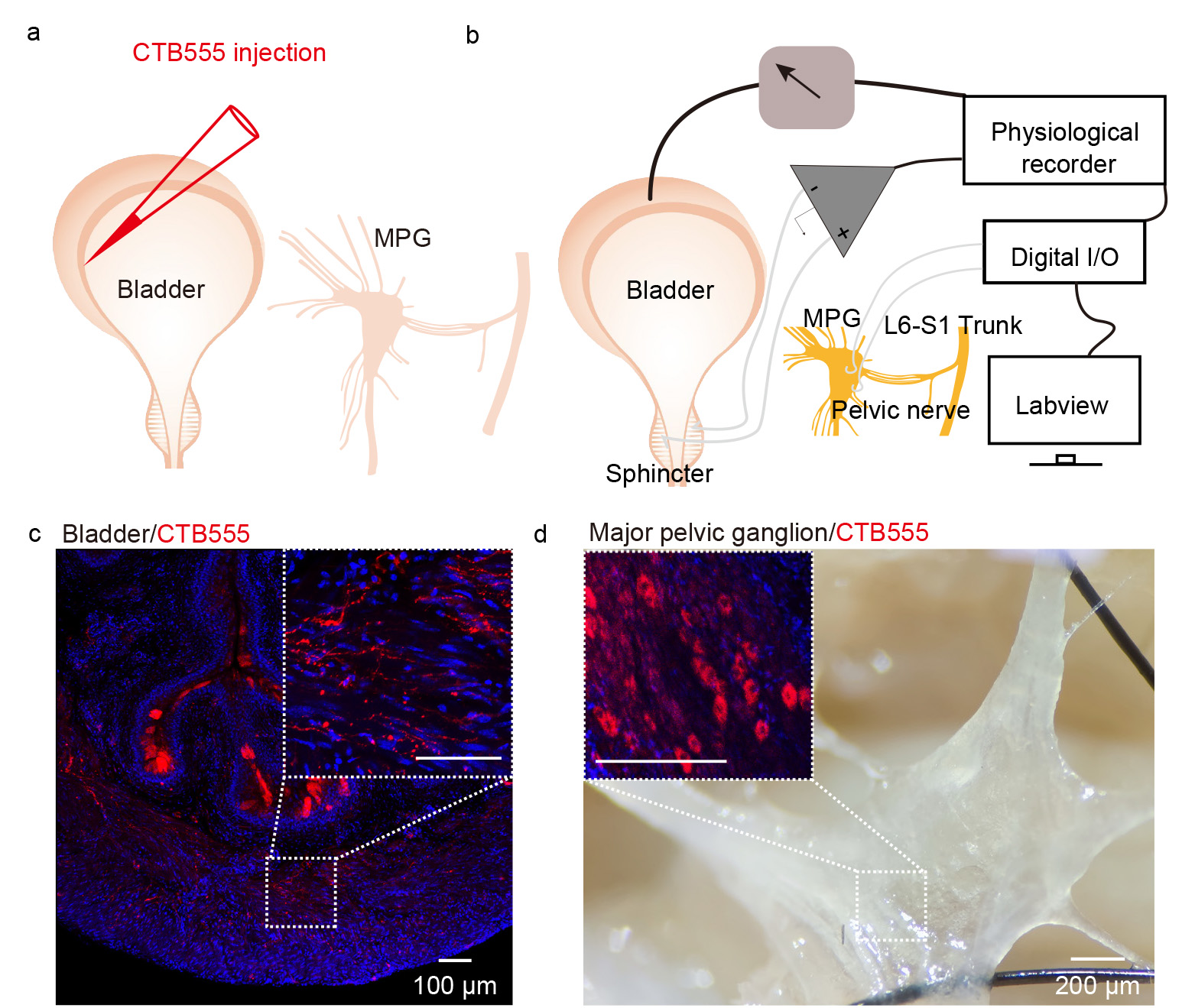
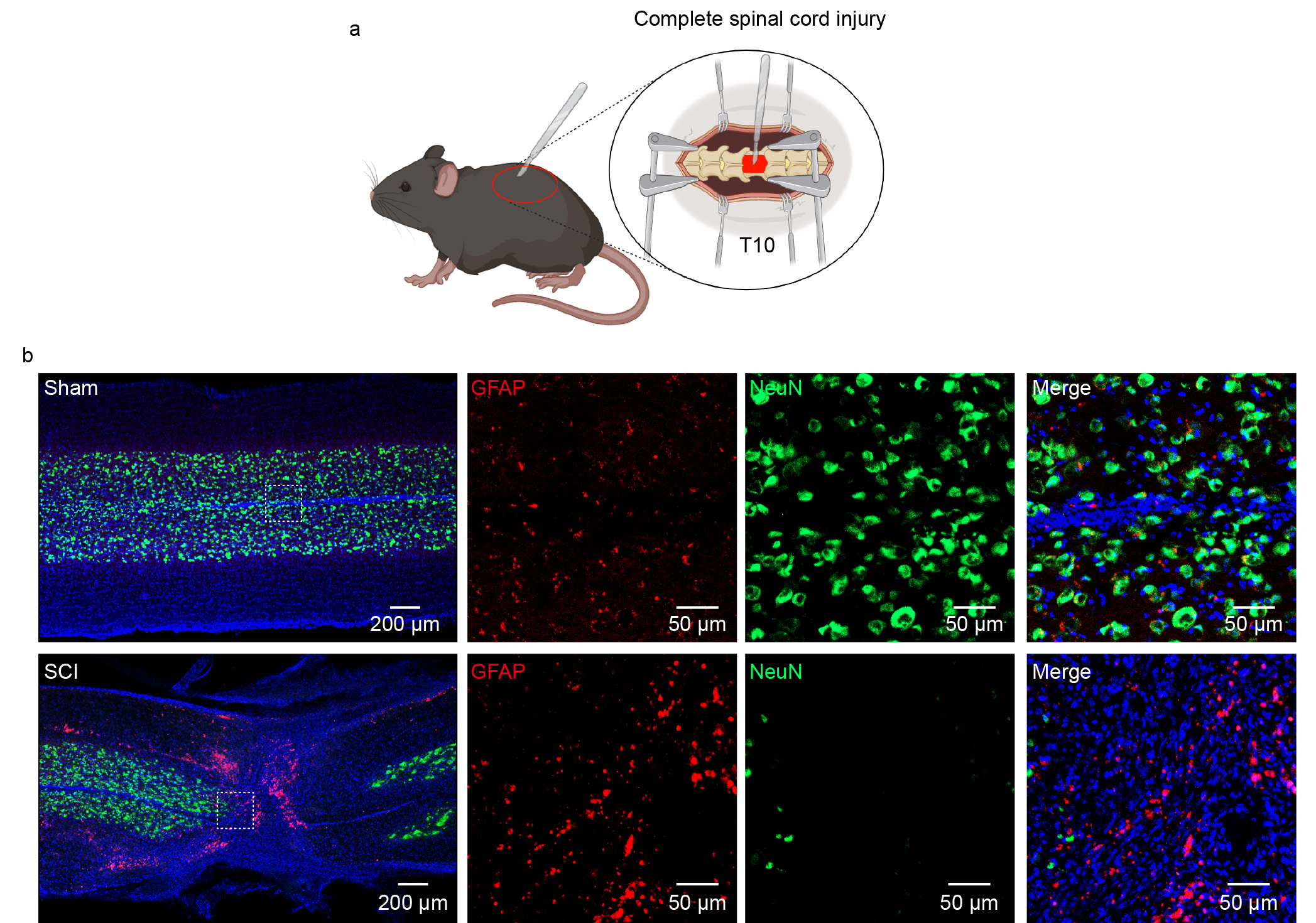
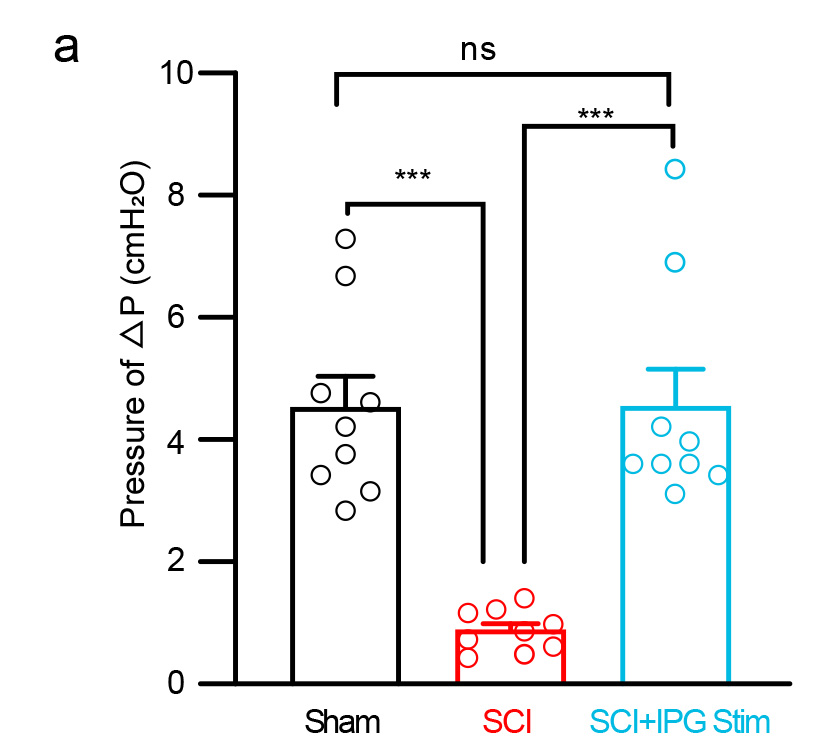
We confirmed both the stimulation and lesion sites to ensure the reliability of the experiment. We injected the CTB into the bladder (Supplementary Fig. 3a,3c,3d) and urethral sphincter (Supplementary Fig. 2a-b) to label the MPG and PN. Post-hoc immunostaining revealed a reduction in the density of NeuN + cells and an increase in the expression of GFAP (a marker of inflammation) at the lesion site in SCI mice (Supplementary Fig. 4b). In subsequent electrical stimulation validation experiments using the SCI model, we obtained results similar to those from the stimulation of intact mice (Fig. 5D). Overall, our results demonstrated that synchronized dual-site electrical stimulation can effectively treat lower urinary tract dysfunction. With the advancement of artificial intelligence and brain-machine technologies, human-machine interaction has become possible. Our study lays the groundwork for future human-machine interactions aimed at achieving artificial coordinated control of the bladder detrusor and EUS.
Our current findings have been validated under specific conditions in mice, warranting further investigation across various animal models, injury sites, and patterns. Additionally, consideration of wireless electrical stimulation could enhance mobility in future interventions. In conclusion, we introduced an innovative electrical neurostimulation approach to mimic reflective urination control. Our study may offer an alternative therapy for addressing NLUTD and enhancing voiding efficiency in patients with SCI.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}