This study is the first prospective cohort study to demonstrate that cell viability measured with a LDH cytotoxicity assay using serum from patients with COPD could be a good predictor of future AECOPD and mortality.
Phagocytosis of apoptotic cells (efferocytosis) is essential to maintain homeostasis of an organism to preserve health. Dysregulation of efferocytosis and accumulation of dead cells are involved in the pathogenesis of chronic inflammatory disease, including COPD20. Apoptotic cells produce “eat me” signals, and these signals are recognized by phagocytes under normal conditions. However, the activity of the phagocytosis signaling pathway is decreased in patients with COPD21, 22. Therefore, an association between developing COPD and impaired clearance of dead cells has been established. Statin, azithromycin, and rosiglitazone enhance phagocytosis and apoptosis in COPD; lovastatin has been studied to restore efferocytotic function in vitro23, 24. However, to the best of our knowledge, only one study reported the effect of efferocytosis dysregulation on COPD severity and exacerbations, showing that impaired macrophage efferocytosis of eosinophils measured using sputum was related to frequent COPD exacerbations19. However, it is unclear whether blood eosinophils could be a robust biomarker for predicting COPD exacerbation. In a recent study of 22,125 patients with COPD from 11 clinical trials, there was no significant association between blood eosinophils and exacerbation rate after adjusting for the previous-year exacerbation history12. This result corresponds with that of the present study, demonstrating that blood eosinophil count was not associated with exacerbation or mortality rates.
We found that the low cell viability group was significantly older, had a poorer quality of life by SGRQ score, a lower proportion of non-exacerbator phenotype, and a higher mortality rate than the high cell viability group. Furthermore, the low cell viability group demonstrated a trend for increased previous-year severe exacerbation history, higher CAT score and eosinophil counts, and shorter 6-min walk test duration; nonetheless, the between-group differences did not reach statistical significance. Furthermore, there were no differences in lung function or type of inhaler used between the two groups. Traditionally, the severity of COPD is classified using predicted FEV1%25. Recently, a new classification system has emerged, called STAR (Staging of Airflow obstruction by ratio), which uses the FEV1/FVC ratio rather than predicted FEV1% to measure the severity of airflow obstruction. The COPDGene study and the Pittsburgh cohort revealed STAR had better discriminative ability for survival and patient symptoms than that of predicted FEV1%26. However, this new classification system has not been studied in other races (such as Asians), albeit being less sensitive to race/ethnicity. In the present study, FEV1/FVC was not significantly associated with exacerbation incidence (adjusted IRR: 0.98, 95% CI: 0.94–1.03) and mortality (hazard ratio: 0.99, 95% CI: 0.97–1.02). In contrast to the STAR system, low cell viability was associated with increased unadjusted and adjusted IRRs of future severe AECOPD risk after adjustment for age, BMI, smoking history, CAT score, SGRQ score, 6-min walk test performance, predicted FEV1%, FEV1/FVC ratio, and previous exacerbation history within 1 year. Interestingly, a history of severe AECOPD in the previous year was associated with an increased unadjusted IRR for moderate and severe exacerbation, while a history of exacerbation was not found to be significantly associated with future moderate or severe exacerbation risk, after adjustment. Past history of exacerbations is associated with future exacerbation risk. This discrepancy could be explained by the limitation of recall bias associated with the history of exacerbation because longitudinal prospective cohort studies have reported that individuals with a similar exacerbation history had markedly varied trajectories of future exacerbation episodes27, 28.
Regarding the type of inhaler used at baseline, the proportion of ICS + LABA (18.3%) and dual bronchodilator (15.7%) was similar. According to the GOLD 2017 guidelines, ICS + LABA is recommended for use in the group stratified by symptoms, lung function, and number of exacerbations or severity, regardless of the eosinophil count29. The use of these inhalers might have influenced the outcomes; however, there was no difference in inhaler type used between the low- and high-cell viability groups.
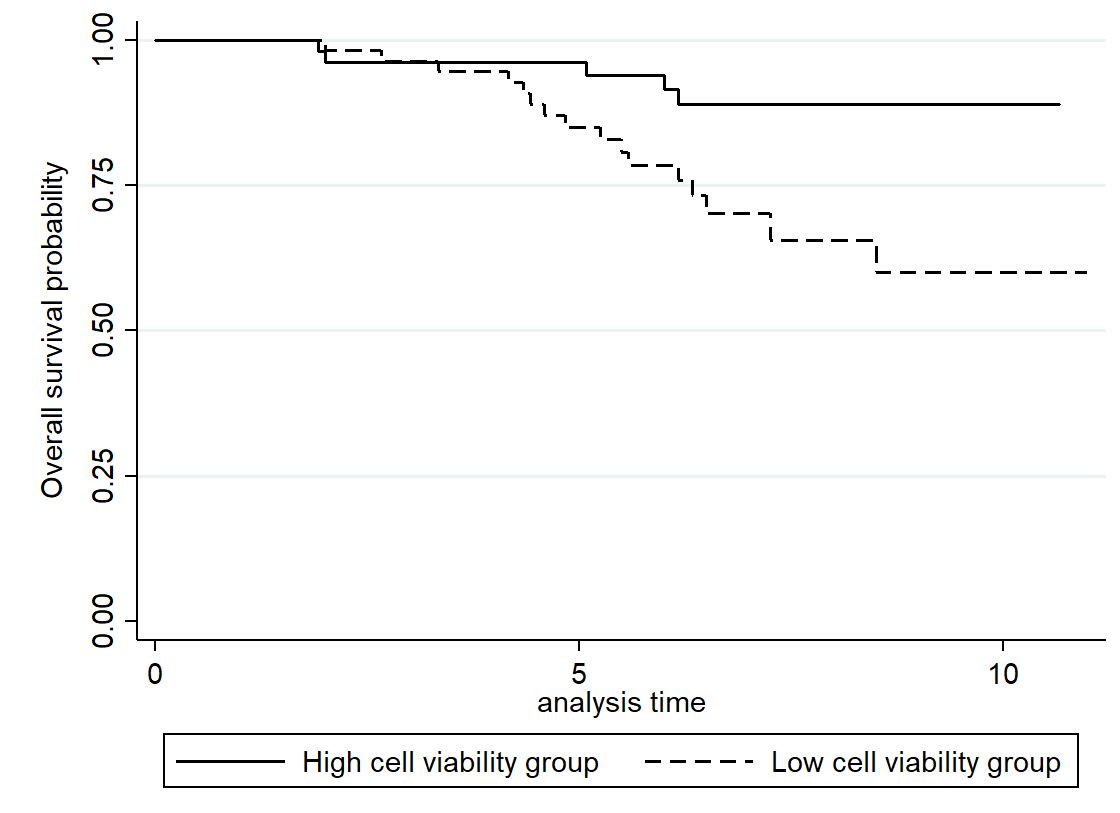
Additionally, our results showed that low cell viability was associated with a 5.79- fold increase in mortality, while a history of exacerbation in the previous year, after adjustment, was not significantly associated with mortality. After the first severe exacerbation event requiring hospitalization, some patients remain stable without further exacerbation; however, after the second exacerbation event requiring hospitalization, there are frequent exacerbations with shorter intervals between them, and the mortality rate increases with each subsequent exacerbation30. The association between cell viability and survival (rather than the history of severe exacerbations) in patients with COPD could be explained by our finding that low cell viability was associated with more frequent exacerbations, leading to rapid deterioration of health status and increased mortality risk.
These findings suggest that low cell viability could be an indicator to identify patients who are more symptomatic, less able to exercise, more likely to have frequent exacerbation events, and have a higher mortality rate, irrespective of lung function and history of severe exacerbations in the previous year.
The present study has several strengths. First, it was the first study to evaluate the value of serum cell viability as a prognostic biomarker for future COPD exacerbation. Second, this was a prospective study with a substantial follow-up period, covering a median of 6.3 years. Third, we analyzed the various clinical parameters and lung function results that could be associated with COPD prognosis. Nonetheless, this study also has some limitations. First, never-smokers accounted for only 3.5% of our cohort; hence, the value of cell viability needs to be validated in patients with COPD without smoking history. Second, serum contains LDH which can decrease the sensitivity of the LDH cytotoxicity assay or detection of cellular LDH. However, we have diluted enough serum concentration mentioned above, so we reduced the high back ground effect as much as possible. Last, the operational definition was used for the degree of cell death due to the absence of absolute reference value of OD for cell viability using serum.
In conclusion, low cell viability measured by a serum LDH cytotoxicity assay was associated with further severe exacerbation and higher mortality in patients with COPD. Further research is needed to validate serum cell viability as a biomarker for COPD exacerbation risk.
{kind=link}