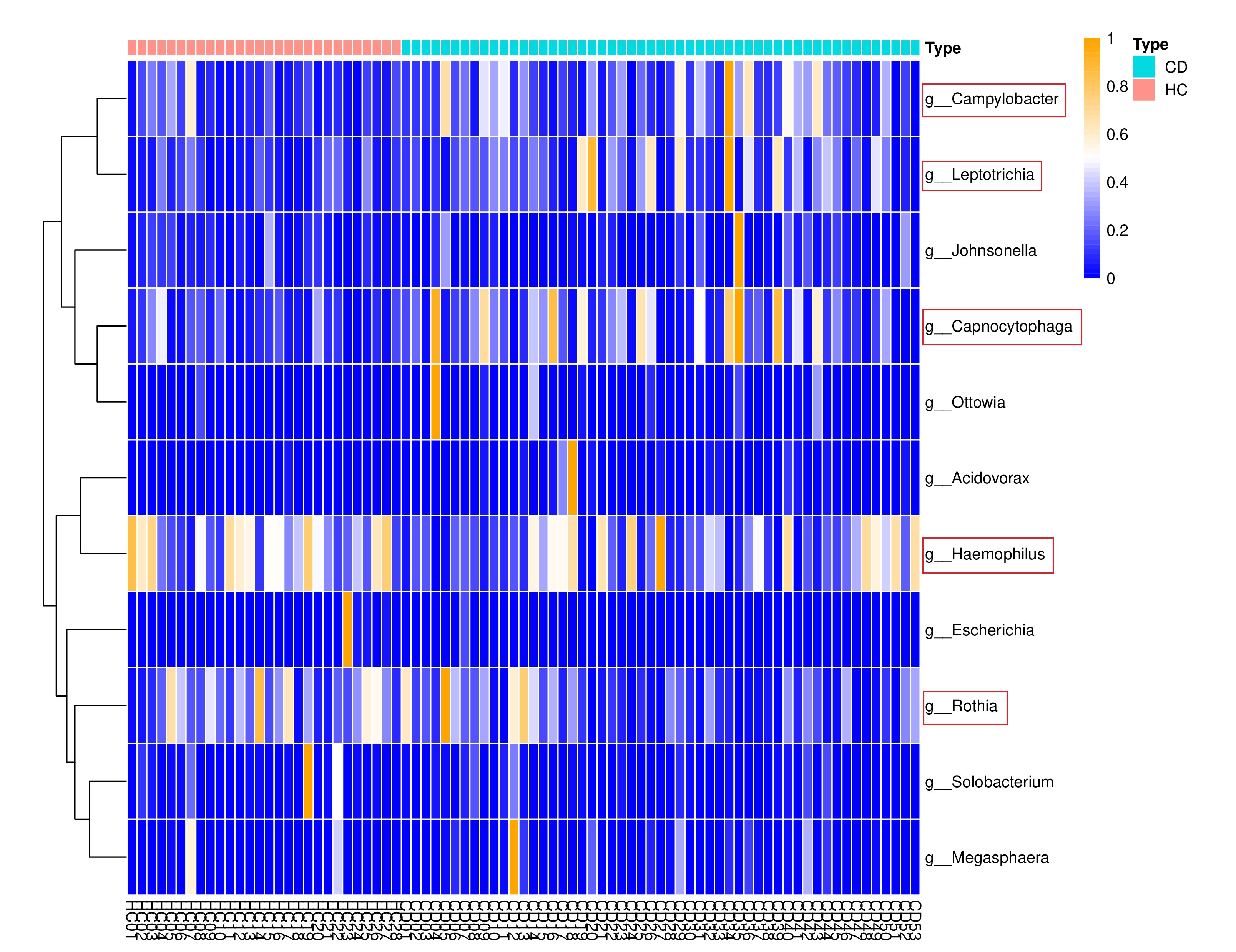
We demonstrated differences in the oral microbiota between healthy individuals and CD patients. Corresponding with the study of Xun, Z. et al. [18] on the oral microbiota composition in CD and HC, at the phylum level, Firmicutes, Proteobacteria, Bacteroidetes, Fusobacteria, Actinobacteria, and Saccharibacteria_TM7 comprised the majority of oral microbial community in CD patients. Compared to healthy controls, the relative abundance of Haemophilus and Rothia was lower in CD patients. Besides, we observed that patients with CD had a higher abundance of Fusobacteria, Leptotrichia, Capnocytophaga, and Campylobacter, suggesting the potential oral microbiota disruption in this particular population.
Since our study, along with the previous research [18], has shown that the composition of microbiota differs between HCs and CD patients, we postulated the difference of oral microbiota also existed among CD patients. To personalize the treatment of CD patients, we further focused on the role of oral microbiota in the efficacy of UST therapy for CD patients.
With the analysis of baseline oral microbiota in CD patients commencing UST treatment, our study revealed the variation in oral microbiota among different clinical efficacy outcome subgroups. The PCoA analysis based on Bray-Curtis proved the different microbial composition between the response group and the nonresponse group, which could be related to the immunoheterogeneity of CD. It is suggested that the oral microbiota of responders to UST is associated with the IL-12/23 related immune response, while the oral microbiota of nonresponders is not. However, there was no significant difference in beta diversity between the nonremission group and the remission groups. It probably could be explained by the fact that some patients who were defined as response did not meet the standard for remission and were therefore classified into the nonremission group. This may weaken the relationship of oral microbial composition and clinical efficacy, when the clinical outcome variable was remission and nonremission.
Accumulating studies have confirmed the role of oral microbiota in prompting intestinal inflammation [27–29]. Due to the multiple barriers of the gastrointestinal tract, oral pathogens can barely colonize in healthy gut environment. However, in patients with IBD, the gastric acidity is attenuated and the intestinal tight junction is damaged, allowing for the ectopic colonization of oral bacteria in gut [19, 30]. With the enteral dissemination, oral pathogens generate lipopolysaccharide (LPS), interleukin (IL) -17, IL-1β,TNF-αand other virulence factors, disrupting the integrity of intestinal barrier and aggravating both intestinal dysbiosis and chronic inflammation [31–33]. In an animal experiment conducted by Atarashi, K. et al. [34], it was confirmed that Klebsiella isolated from the saliva has the ability to colonize the gut and induce significant gut inflammation through the activation of Th1 cell. Additionally, oral bacteria can spread through the blood stream during dental procedures such as toothbrushing and dental extraction [35, 36]. Upon entering the systemic circulation, these oral pathogens stimulate dendritic cells and macrophages, consequently modulating the microenvironment of the gut microbiota through the induction of host immune responses. [28, 37] .
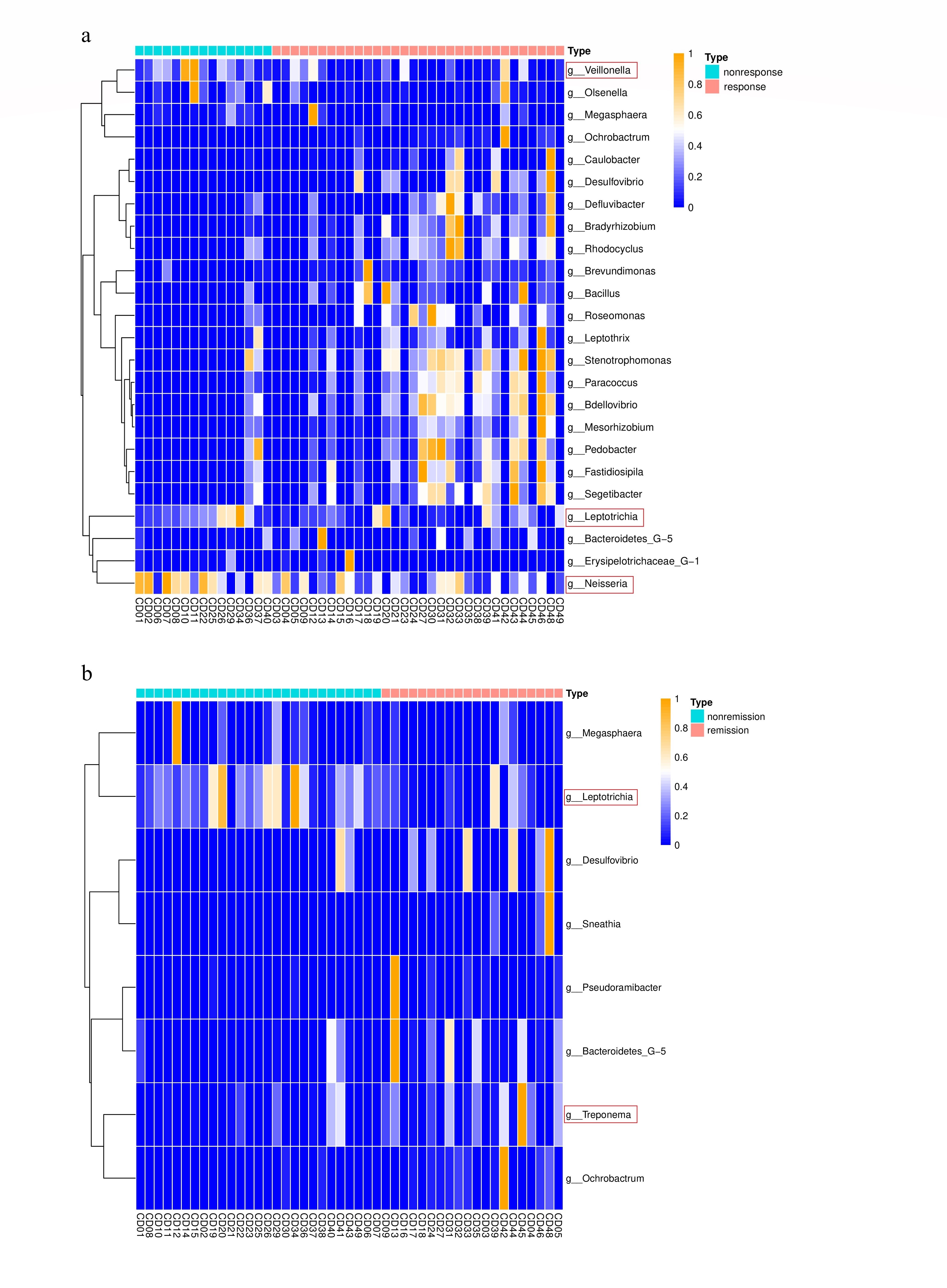
Moreover, while conducting the LEfSe analysis, a higher abundance of Fusobacteria and Leptotrichia was found to be associated with the loss of response to UST in CD patients. Notably, the enrichment of Fusobacteria and Leptotrichia was also observed in the nonremission group, when compared to the remission group. And metabolic functional variation prediction analysis showed the energy metabolism pathway and metabolism of cofactors and vitamins pathway were enriched in the nonresponse group. Above all, our findings suggested that oral microbial composition might be related to the efficacy of UST in CD.
Fusobacteria are anaerobic, Gram-negative bacilli, and frequently found in the human oral cavity, comprising two families, Leptotrichiaceae and Fusobacteriaceae. The enrichment of Fusobacteria has been observed in the colonal biopsies of IBD and in the fecal microbiota of severe pediatric ulcerative colitis [15, 38]. Besides, it has been found that a higher abundance of Fusobacteria is related to the postoperative disease recurrence in patients with CD [39]. Prior researches of CD-associated Fusobacteria are mainly focused on Fusobacterium nucleatum. F. nucleatum is traditionally well known as periodontal pathogen, prompting the structure of dental plaque biofilm [40]. It is rarely detected outside of the oral cavity in healthy individuals, but is present in the gut of people with IBD and colorectal cancer [41, 42]. Engevik, M. A. et al. [27] proved that in gut dysbiosis mice, F. nucleatum secrets outer membrane vesicles to promote intestinal inflammation. Another research on colitis mice model discovered that F. nucleatum produces FadA, an adhesion, which contributes to the acidresistance of F. nucleatum under disease conditions. This, in turn, prompts the colonization of F. nucleatum in gut environment [43].
Leptotrichia is also within Fusobacteria. It is considered as an opportunistic pathogen that can be found in the oral cavity, intestinal tract, and urogenital system of humans [44]. It has been reported that Leptotrichia is related to septicemia in patients with mucositis, oral lesions, wounds, and abscesses [45, 46]. A recent observation has confirmed that the enrichment of Leptotrichia in the intestinal environment of UC [47]. Another 10-year retrospective clinical study indicates that Leptotrichia is associated with invasive infections, particularly among immunocompromised patients [48]. Langfeldt, D. et al.[49] found that Leptotrichia could induce the transcription of proinflammatory factors including IL-1β, IL-6, IL-8, and IL-10 in epithelial cells. The enrichment of Fusobacteria and Leptotrichia was found related to a lower risk in pancreatic cancer. The researchers assumed that it could profit from the immune response elicited by Leptotrichia, providing the protection against pancreatic carcinogenesis [50]. It’s likely that this possible immune mechanism, which is associated with reduced risk of pancreatic cancer, induces an autoimmune response in patients with CD, thus exacerbating intestinal inflammation. Fusobacteria and Leptotrichia could be considered as potential therapeutic targets of CD. However, further investigations are needed into the pathogenesis of Leptotrichia and other species of Fusobacteria in gastrointestinal diseases.
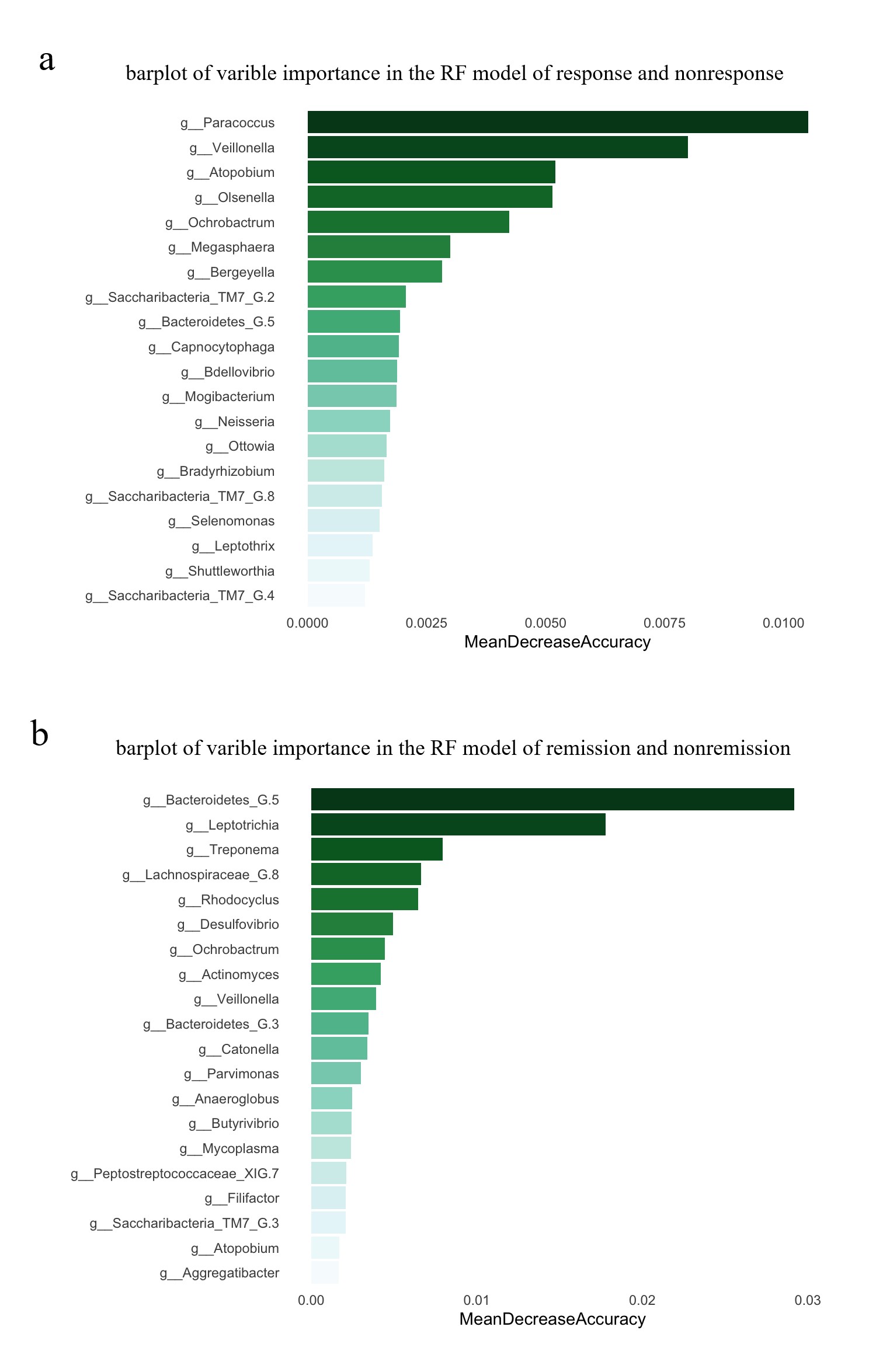
Furthermore, we constructed RF models to predict UST efficacy in CD. The AUC for the predictive model which distinguished responder and nonresponder was 0.944, while the AUC for the model predicting clinical remission was 0.930. The results suggested that the oral microbial composition showed a great ability to classify CD patients with different UST efficacy. Our study was the first to verify the association of oral microbiota and the clinical outcome of UST in CD. It may allow the identification for CD patients with a higher likelihood of UST response based on oral microbiota. Moreover, compared to fecal microbiota and mucosal biopsy, the sample of oral microbiota is non-invasively and easily obtainable. If the classification model could be applied in larger cohort, it will help instructing the treatment of UST in CD.
Nevertheless, our study has some limitations. Our research, as a single-time point research, cannot reveal the causality between the oral microbiota composition and the efficacy of UST in patients with CD. In order to minimize the effect of diet on the composition of oral microbiota, we recruited the patients’ family members as controls. However, family members may share genetic predispositions or environmental factors with CD patients, leading to similarities in oral microbiota composition that could narrow the differences between CD patients and healthy controls. Moreover, there still exists potential confounding factors such as oral hygiene behaviour and socio-economic factor which we did not taken into account. By focusing on the top 5 genera, our random forest analysis may understate the nuanced relationships and interactions between different microbial species. Due to the lack of researches related to the association of oral microbiota and UST efficacy in CD, a larger randomized cohort would be desirable to confirm the variations in the oral microbiota and its predictive ability as a biomarker in CD patients treated with UST.
{kind=link}
{kind=link}
{kind=link}
{kind=link}