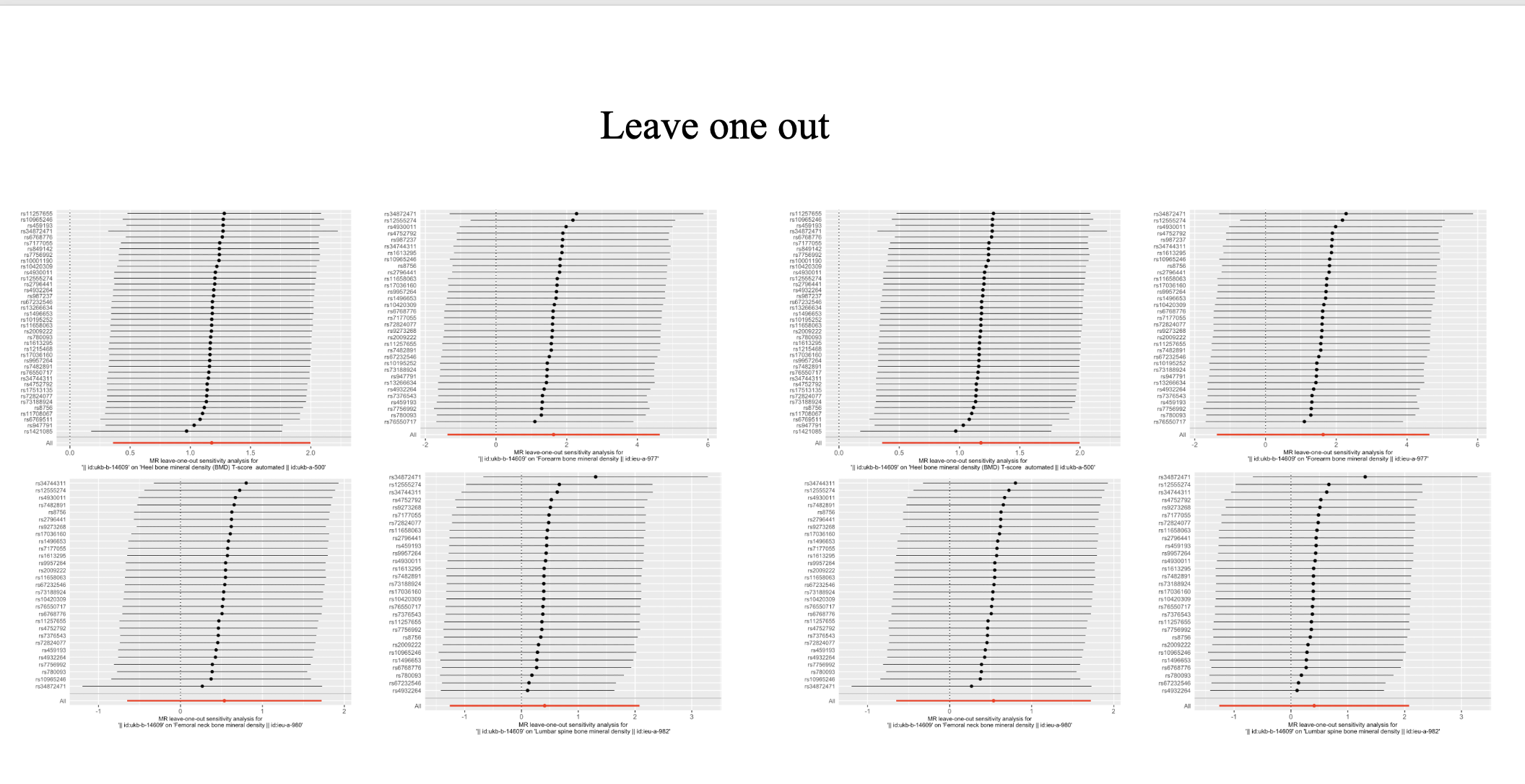
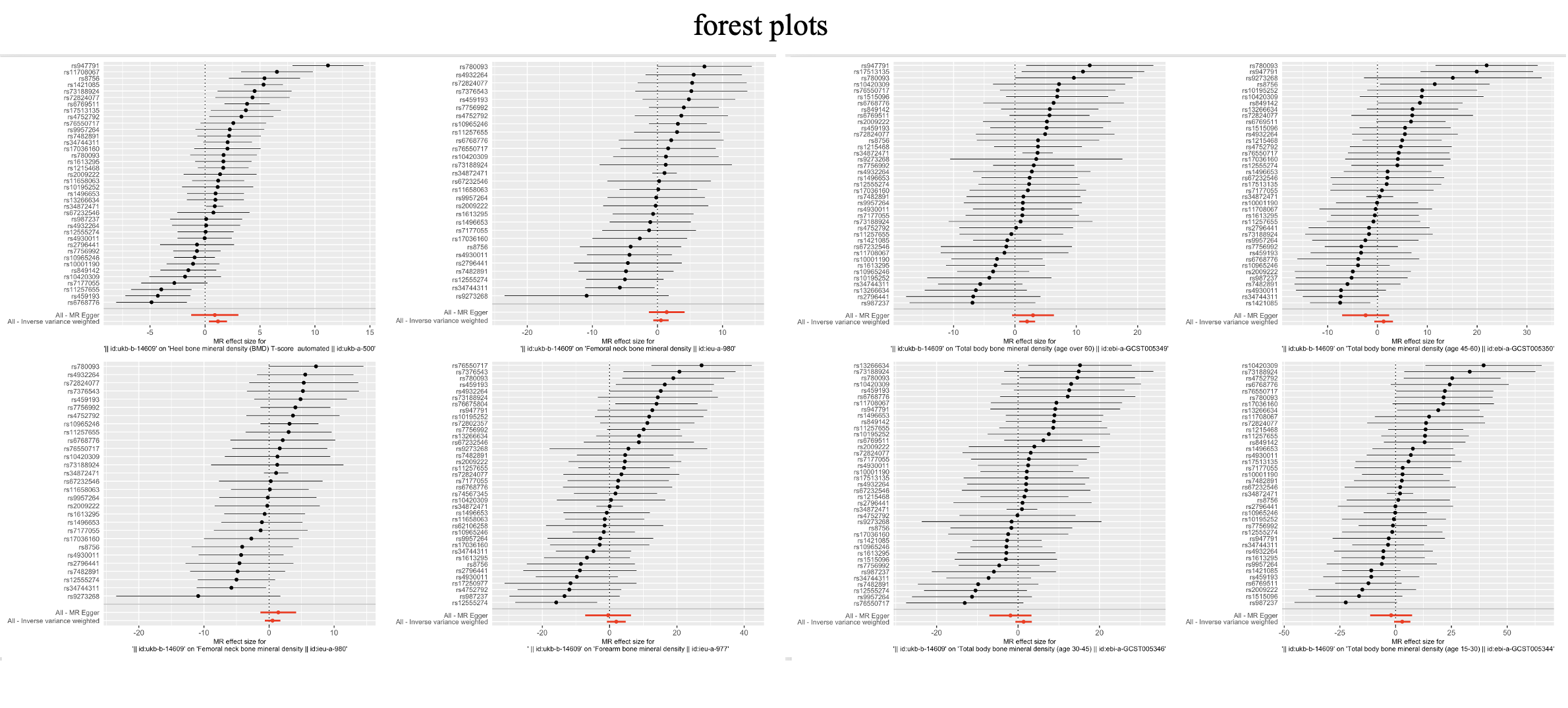
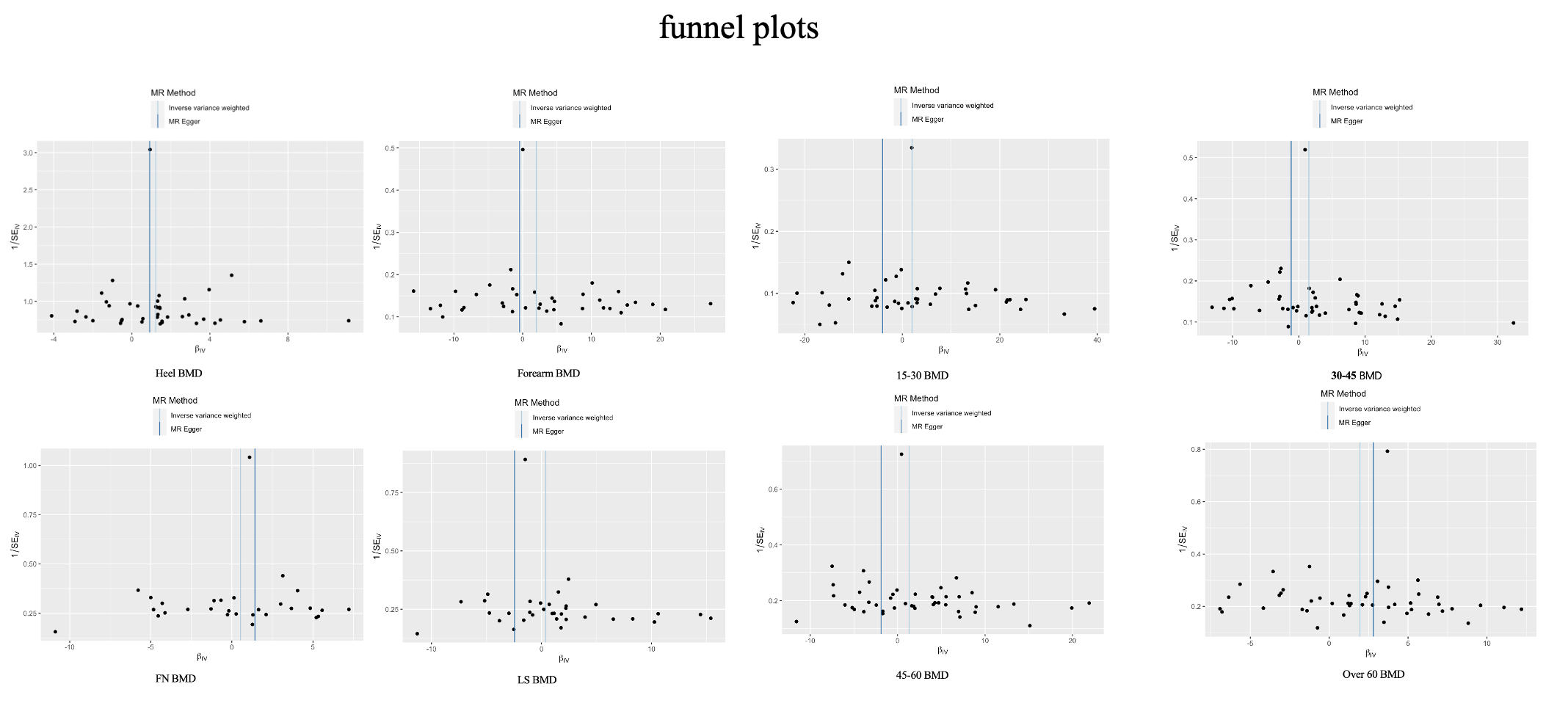
In this study, we determined whether there is a causal relationship between metformin and BMD using the MR method. Through the public GWAS summary database, in general, we did not find a causal relationship between metformin use and increased BMD. However, there is a causal relationship between metformin use and elevated heel BMD, and there are also indications that metformin use is associated with elevated BMD over the age of 60 years. The results of the sensitivity tests support these conclusions.
Diabetes and osteoporosis are generally regarded as separate diseases in clinical practice, but they have been associated in epidemiological studies in recent years18,30. A growing body of evidence suggests that there is a pathology between diabetes and osteoporosis. Examples include impaired bone strength due to low bone turnover, inflammation, dysregulation of the Wnt signaling pathway, and bone marrow fat accumulation due to obesity31. Osteocalcin is a marker of bone remodeling in the circulatory process of bone metabolism, and serum osteocalcin levels are associated with osteogenesis32. O'Berezovska et al. found lower bone mineral density in mice with the osteocalcin knockout phenotype33. It has been shown that osteocalcin expression is decreased in all diabetic patients34,35. In addition, diabetes-induced abnormalities in the expression of adipokines have been associated with the development of osteoporosis. Adipokine has been shown to correlate with systemic insulin sensitivity in humans positively and is reduced in diabetic patients36. In vitro studies show that adipokines inhibit inflammatory gene expression and promote osteogenic differentiation of hPDLCs (human periodontal ligament cells) via the NF-κB pathway37. Leptin (a hormone secreted by fat cells) regulates energy metabolism and controls inflammatory factors38. Leptin induces the differentiation of skeletal stem cells (the source of osteoblasts and adipocytes) into adipocytes through activation of Jak2/Stat3 signaling, and Yue et al. found that rat limb bones exhibited enhanced osteogenesis and accelerated fracture healing by knocking out the leptin receptor (LepR) in bone marrow stromal cells of the limbs39. The Wnt signaling pathway, which promotes osteogenesis, was observed to be inhibited in patients with T2D in a clinical study by Leanza et al. and is likely to be associated with the expression of sclerostin, as well as a link between the production of advanced glycosylation end-products (AGEs) in response to high blood glucose levels and high sclerostin activity40. AGEs also activate multiple inflammatory signaling pathways, such as MAPK/ERK, TGF-β, and NF-κB, enhancing inflammation and inhibiting bone formation41.
Metformin is heavily used as a first-line agent in treating T2D. The potential application of metformin has been discussed in recent years. Marc Foretz et al. discuss new therapeutic uses for metformin based on newly identified targets of metformin's action in recent years, including involvement in COVID-19, management of body weight, and targeting brown adipose tissue for functionality42. AMPK is an enzyme that plays a role in cellular energy metabolism43. There is evidence that metformin inhibits complex I of the mitochondrial respiratory chain, which leads to an elevated AMP/ATP ratio to increase AMPK activity44,45. AMPK can promote the transformation of MSCs(mesenchymal stem cells, progenitors of adipocytes, and osteoblasts) into osteoblasts by regulating the Wnt/β- catenin pathway46. MSCs can also differentiate into osteoblasts through the induction of Runx2, a major transcription factor for osteogenesis, and AMPK promotes Runx2 expression47. MSCs are induced by peroxisome proliferator-activated receptor-γ (PPAR-γ) to differentiate towards adipocytes, while osteoblast differentiation is inhibited47. Chyau et al. showed that AMPK can work with Sirt1 to inhibit PPAR expression and thus inhibit lipid synthesis.48 Osteoprotegerin (OPG) is a tumor necrosis factor regulated through the nuclear factor kappa-B ligand(RANKL)/nuclear factor kappa-B(RANK)/OPG pathway, which effectively inhibits osteoclast differentiation and maturation, and participates in osteoblast differentiation and bone formation49,50. PPARγ-1 can activate RANKL signaling to increase osteoclast expression and enhance bone resorption. A cellular study by Zheng et al. found that inhibition of PPAR by carnosic acid led to inhibition of estrogen-associated receptor alpha, which resulted in inhibition of RANKL to reduce osteoclast formation and ameliorate bone loss51. Metformin reduces the production of AGEs through its hypoglycaemic effect, thereby reducing bone destruction caused by the inflammatory response41. In addition, the experiments of Zhou et al. found that metformin also inhibited the reduction of AGEs production through AMPK activation and RAGE/NF-kB pathway52.
Although the present study did not find a clear causal relationship between metformin and BMD, we observed a potential effect of metformin on BMD on some of the results. The changes in BMD imply that metformin improves OP not only by controlling blood glucose levels to reduce inflammation or by regulating lipid metabolism but also by promoting osteoblast expression directly through relevant signaling pathways42. For people with diabetes, especially type 2 diabetes, taking metformin can bring about a preventive effect against osteoporosis, thereby reducing the risk of fractures and improving quality of life. On the other hand, the observed modulation of bone metabolism-related pathways by metformin in animal or cellular experiments may allow it to be involved in non-diabetic osteoporosis, which needs to be further verified by clinical trials.
{kind=link}
{kind=link}
{kind=link}