Comprehensive NGS sequencing is becoming a common approach for upfront assessment of a broad range of genetic biomarkers that are pivotal for diagnostic, prognostic, and therapeutic decisions in cancer patients. While ideally, molecular testing is greatly facilitated when large tumor samples are available (i.e. resections or excisional biopsies), the reality of clinical practice is that a very large proportion of testing must be performed on scant material obtained through minimally invasive procedures. Historically, this has presented distinct challenges, prompting the adoption of alternate approaches, such as liquid biopsies, which attempt to circumvent tumoral cell assessment altogether. At present, while arguments can be made for the superiority or inferiority of each modality over another, cytologic samples stand as the one middle approach that unites the most desirable attributes of both worlds. Namely, they retain the key morphologic correlates required for tumor diagnosis, while still sparing the patient from the more invasive procedures. One fact remains constant, however, which is that small samples require very high optimization of the entire process to maximize the genomic yield.
In this study, we have outlined our institutional approach and longitudinal experience in comprehensive profiling of cytology samples in routine clinical care. To our knowledge, this represents the largest prospective clinical cohort reported to date, demonstrating that molecular testing can be performed on routinely procured cytology samples with high success rates, similar to surgical samples. Proportions of clinically actionable genomic alterations, specifically OncoKB Level 1–3B, as well as R1 alterations, recapitulated the expected patterns across all tumor types when compared to those published in AACR GENIE cohort. For immediately actionable alterations (OncoKB Level 1), the concordance of cytology to corresponding surgical samples from the same patient were very high (93%). Notably rescue ScfDNA from supernatant CytoLyt fluid material, utilized for our internal cases, proved highly valuable and enabled the detection of a level 1 alteration in 83% of the successfully sequenced cases.
Our review of data compiled across 8 years, highlighted the central roles of optimized sample handling and processing. In our hands, 2 critical early steps enabled higher DNA recovery which, consequently, promoted increased utilization of cytologic material for molecular testing. The first was the optimization of cell block preparation, which incorporated pretreatment of pelleted cells with 95% ethanol before addition of HistoGel12,13. This enhanced the density of cell pellets to deliver higher amount of cellular material in fewer sections of the paraffin block. The second was the transition to mineral oil deparaffinization which markedly reduced tube transfers, centrifugation, and decanting steps, all key vulnerabilities responsible for major nucleic acid losses in the processing of scant FFPE material14–16. It should be noted that, with the implementation of mineral oil extraction, requests for testing on cytologic material vs needle biopsies markedly increased at our institution. Details of this transition have been previously published by our group16,20. Notably, among lung cancer patients undergoing endobronchial ultrasound transbronchial needle aspiration (EBUS-TBNA) this change, alone, significantly improved sequencing success rates from 76.3–93%. Moreover, these success rates corresponded to NGS testing that was performed after standard rapid testing for EGFR on the same samples21, further supporting the high suitability and sufficiency of the DNA recovered.
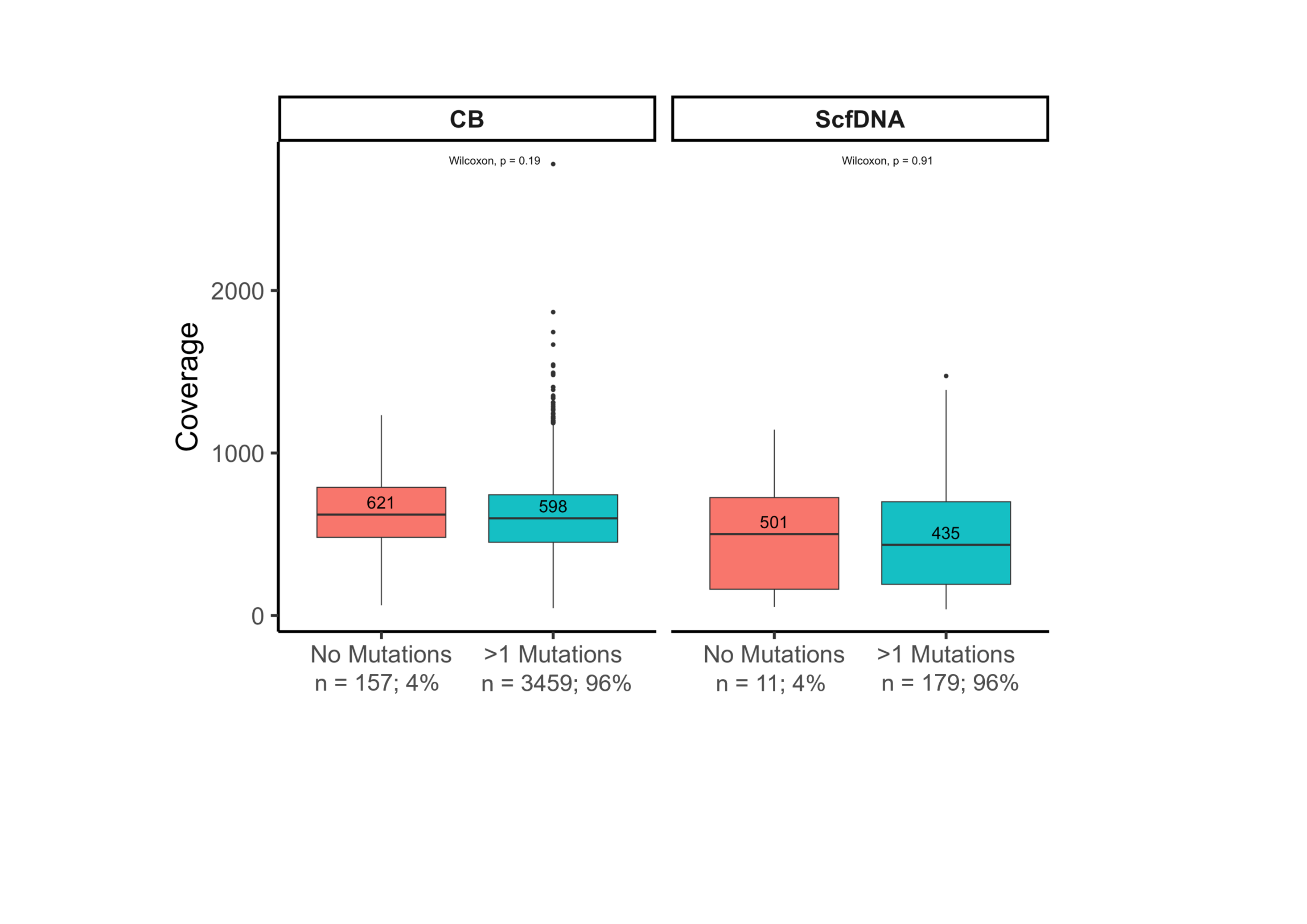
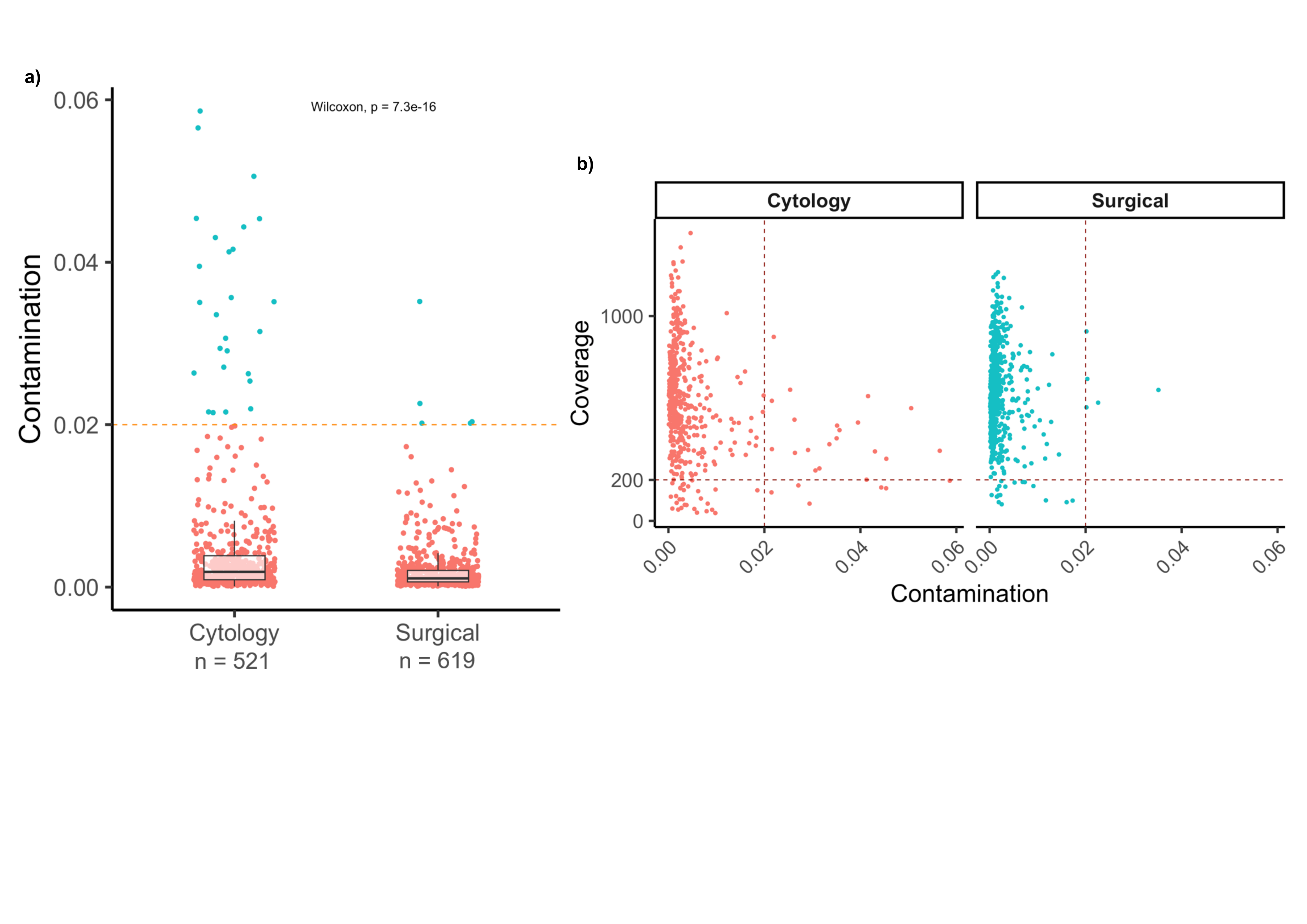
An important, and often underreported, consideration in molecular testing of cytology samples are the diagnostic challenges and inaccuracies that may arise from sample cross-contamination. While sample-to-sample contamination may happen across any point, highly vulnerable points lie in processes that involve batching and pooling of multiple samples in a single run. In particular, established histopathology practices of tissue processing (i.e. carry over from microtome blades, common water baths, pooled tissue processors, etc.), pose distinct risks for contamination for small tissue samples as processes are primarily optimized to enhance microscopic diagnostic analysis but not downstream molecular applications. Common holding of numerous specimens in single chambers in automated tissue processors, the use of common equipment for embedding, cutting and tissue mounting, all increase the potential for low level cross contamination. While this may remain inconsequential for morphologic assessment or the molecular analysis of large tissue samples, this can distinctly impact small samples where similar contamination levels become proportionally higher. Cytology samples may be even more vulnerable due to processing of cell blocks with paper wrapping and HistoGels, which may promote trapping of cellular impurities from other samples. Indeed, in our analysis of cytologic samples, contamination was significantly higher across CB samples compared to all other samples. This held true when analyzing samples with adequate coverage (> 200x) with 4% of CB samples exhibiting contamination. ScfDNA samples by contrast, which are processed individually in a closed system and not batched, had negligible levels with contamination patterns exclusively associated with sequencing failures or borderline coverage and more likely related to artifact rather than true contamination. Despite the presence of higher contamination levels in cell blocks, the overall rate was low (4.8%) among successfully sequenced samples, which encompassed samples procured and processed across numerous laboratories across the county. These rates are in keeping with sequencing data on surgical samples published by Sehn et al22 but are significantly lower to what is reported by the ASC Clinical Practice Committee/Workgroup for Cross-Contamination in a recent survey for general cytopathology practice, quoting rates as high as 56% for cell-block preparations23. This high rate may be related to the reporting of contamination per case, affecting some but not all unstained sections and which may not be high enough to be detectable in the sequencing of DNA recovered from a set of several slides. Importantly, while contamination was detectable in several cases in our cohort, most were sufficiently low in comparison to the overall tumor content of the sample, allowing informed filtering of low–variant allele fraction events without compromising all mutation calling. In all, only 1.3% of the samples were failed due to contamination, while others could be reported with modification. Within the molecular laboratory, a notable source of cross-contamination may arise from index-hopping during multiplexing. This, however, is generally lower level (well below 2%) and more prone to affect higher sensitivity applications. Nonetheless, in the process of improvement for our MSK-IMPACT assay we have incorporated several strategies to mitigate this phenomenon, including optimization of PCR conditions and the implementation of dual indexing to facilitate the removal of misaligned reads. These finetuning steps facilitated our decision to reduce the assay input requirements which markedly reduced failures due to insufficient DNA. No significant changes in coverage or contamination rates were seen with this change.
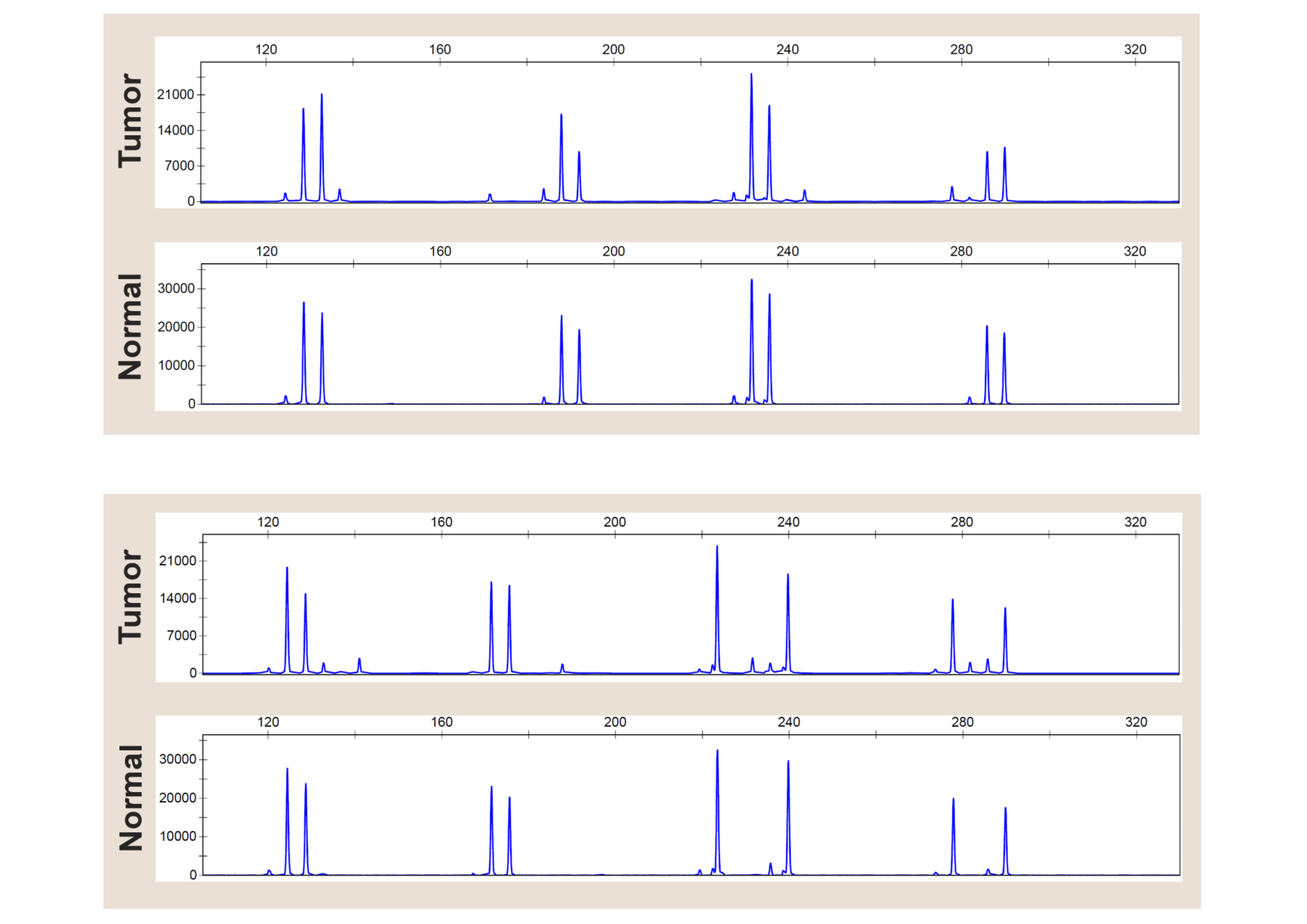
Finally, a pivotal component of our optimization process was the implementation of testing ScfDNA recovered from liquid cytology preparations. While, generally, this sample type was not submitted if the cell block was deemed suitable for testing, it became an important rescue sample to avoid re-biopsy procedures. The use of this material also relieved some of the challenges in triaging very small biopsy samples for other ancillary studies. In all, while the success rate of the ScfDNA samples was approximately 71%, which is below what is seen across tissue biopsies and CB, these samples were specifically tested after the corresponding cytologic material was deemed unsuitable, thus boosting the overall success for the individual aspirate procedures by approximately 3%. An important observation, gathered from the comparison of ScfDNA and corresponding cell blocks, is that the VAF’s of detected alterations were similar for both preparations, supporting that the assessment of the block or cytoprep represents a suitable surrogate for estimating the proportion of tumor derived DNA that may be present in the ScfDNA sample. Additionally, given the high integrity of the DNA in these non-formalinized samples, lower DNA inputs still delivered excellent results, provided that the tumor proportion was suitable. Confirmatory testing with higher sensitivity methods may also be implemented for low tumor samples, without concerns for false positivity due to artifacts imparted by formalin fixation.
In conclusion, this study confirms that the routine use of cytologic samples for molecular testing constitute a robust approach that can deliver the same results as larger biopsy samples. Process optimization and the implementation of robust quality control processes, including contamination checks are pivotal to maximizing the yield and utility of these samples. A reassessment on how tissue blocks are processed and prepared would be an important aspect of cytology practice as a whole, to include specialized instrumentation for processing small samples without risk of cross-contamination. ScfDNA recovered from supernatants is an invaluable source of tumor derived DNA which circumvents the processing where most contamination is bound to happen in current practice, and while failure rates due to limited nucleic acid recovery are higher than tissue blocks, their use could rescue the majority of cases where high tumor is identified but FFPE material is insufficient for sequencing.
{kind=link}
{kind=link}
{kind=link}