Baseline Characteristics
In total, 182 CDIF patients and 22,845 CD patients were followed for 2,283 and 293,537 patient-years, respectively.
At CD diagnosis, CDIF patients had a lower median age than CD patients (24, IQR 17.2–34.8 vs 35, IQR 23–55). A greater proportion of CDIF patients (n = 130, 71.5%) were diagnosed with CD before 1991, compared to CD patients (n = 3,770, 16%, p < 0.01), and a greater proportion CDIF patients (n = 156, 93%) had no comorbidities, compared to CD patients (n = 18,173, 80%, p < 0.01).
Cumulative Incidence and Lead Time of Developing IF from CD
New CDIF patients increased every decade until 2010, after which the number plateaued. Despite this, the 10-year cumulative incidence of developing IF in newly diagnosed CD patients decreased from 2.7% prior to 1980 to 0.2% after 2000 (p < 0.01) (Fig. 1), as the number of newly diagnosed CD patients significantly increased in every decade (Table 1).
The cumulative incidence of developing IF was higher in CD patients with younger onset compared to those with mature-age onset, with a 10-year cumulative incidence of developing IF of 0.7%, 0.5% and 0.2% for CD patients with Montreal classifications A1, A2 and A3, respectively (p < 0.01).
The median duration of CD until IF onset (lead time) in CDIF patients was 14.5 years (IQR 8–24). Lead time increased in every decade, from a median of seven years before 1980 to 25.5 years after 2010 (Fig. 2).
CD-related Medication Use
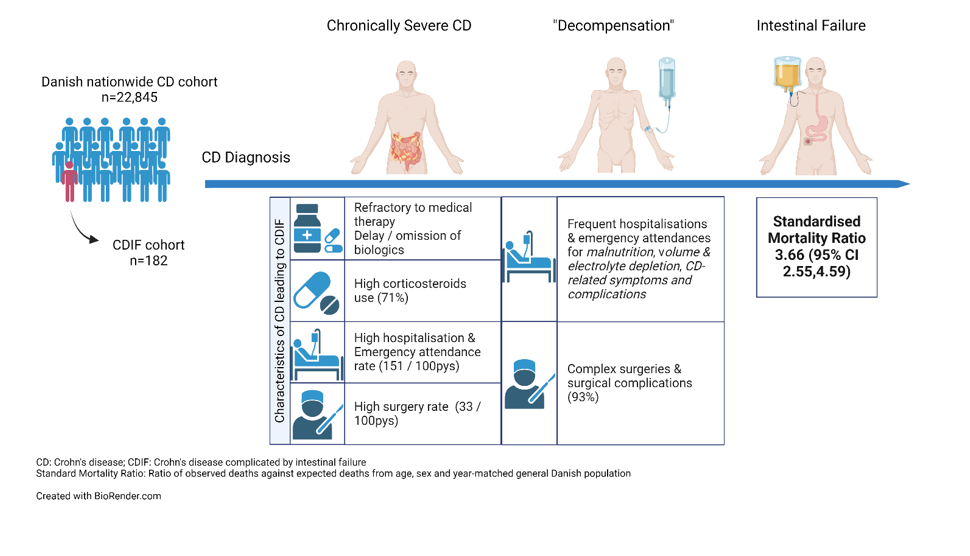
In total, 113 (62%) CDIF and 21,857 (96%) CD patients had all or part of their follow-up after 1995, when data on dispensed outpatient medicines was available. Compared with CD patients, a greater proportion of CDIF patients received corticosteroids (71% vs. 60%, p = 0.02) and immunomodulators (59% vs. 49%, p = 0.03). The proportion of patients exposed to biologics was not different between the two groups (20% vs. 21%, p = 0.95). Twenty-three percent of CDIF and 30% of CD patients received none of the above medications during follow-up (p = 0.12).
In patients who received medications, the cumulative time on biological therapy was shorter among CDIF patients than CD patients (2,068 vs. 4,126 days per 100 patient-years, p = 0.02). In addition, the time from CD diagnosis to first exposure to a biologic was significantly longer in CDIF patients, at 15.4 years (SD 9.2), than in CD patients, at 5.6 years (SD 7.4), due to a higher proportion of CDIF patients whose CD onset preceded the availability of biological therapy.
In patients who received medications, no significant difference was observed between CDIF and CD patients in the mean yearly dose of corticosteroids, the number of years where at least one tapering course of corticosteroids was received, the number of years where any immunomodulator was received, or the number of courses of biologics received (Table 2).
All CDIF patients and 99.5% CD patients received an anti-TNF agent as the first-line biologic. Eighty-three percent of CDIF patients and 94% CD patients stayed in the same class of biologic during follow-up. While 30% of CDIF and 31% of CD patients continued their first biologic beyond three months, CDIF patients were less likely to continue their first biologic for more than a year, at 17% compared to 39% for CD patients (p = 0.06).
Unplanned Inpatient Contacts
Hospitalisation data were available in 168 (92%) CDIF patients and 22,845 (100%) CD patients, who were followed from 1977 to 2018. We identified 8,269 episodes and 171,159 episodes of unplanned inpatient contacts in CDIF and CD patients, respectively, corresponding to 47.3 episodes and 7.94 episodes per patient. Among CDIF and CD patients, 49% and 25% of inpatient contacts were IBD-related (p < 0.01), respectively, and 92% and 70% of these inpatient contacts were admissions (p < 0.01).
Compared with CD patients, a higher proportion of CDIF patients had at least one episode of IBD-related inpatient contact (98% vs. 55%, p < 0.01) during follow-up. CDIF patients had a higher rate of IBD-related inpatient contact (93 vs. 15 episodes per 100 patient-years, p < 0.01), a greater number of follow-up years with at least one IBD-related inpatient contact (93 vs. 15 years per 100 patient-years, p < 0.01), and a higher rate of all unplanned inpatient contacts (150 vs. 58 episodes per 100 patient-years, p < 0.01).
CDIF patients and CD patients showed a downward trend for IBD-related inpatient contacts over time, from 169 episodes and 80 episodes per 100 patient-years before 1980, to 72 episodes and seven episodes per 100 patient-years after 2010, respectively (Fig. 3). IBD-related inpatient contacts declined faster among CD patients than CDIF patients, such that CDIF patients were 2.12 times more likely to have an inpatient contact prior to 1980, and 9.68 times more likely than CD patients after 2010.
On the other hand, non-IBD-related inpatient contacts increased over time among CDIF patients, from 43 episodes to 127 episodes per 100 patient-years, but remained stable among CD patients. This increase was driven by CD-related complications and a reduction of intestinal function in the late stages of CD prior to onset of IF. A pattern of “decompensation” was observed in CDIF patients one year prior to IF onset, with an increase in both IBD- and non-IBD-related inpatient contacts (Supplementary Results). A review of the discharge codes of non-IBD-related inpatient contacts within a year of IF onset showed that 32.7% of these contacts were due to “volume and electrolyte disturbances” or “malnutrition”, and a further 26.8% were due to complications or symptoms that were likely related to IBD or IBD surgery (Supplementary Results).
CD-related Abdominal Surgeries
From 1977 to 2018, we identified 1,234 CD-related abdominal surgical procedures in 168 CDIF patients and 33,475 procedures in 22,845 CD patients. Of these procedures, 529 (42.9%) in CDIF and 13,308 (39.8%) in CD were resections.
Compared to CD patients, a significantly higher proportion of CDIF patients underwent at least one CD-related abdominal surgery (99% vs. 48%, p < 0.01), resection (95% vs. 37%, p < 0.01), or colectomy (84% vs. 33%, p < 0.01) during follow-up. The rate of CD-related abdominal surgeries and bowel resections was higher in CDIF patients (33 and 23 per 100 patient-years, respectively) than in CD patients (8 and 5 per 100 patient-years, respectively, p < 0.01).
In patients who underwent surgery, a higher proportion of CDIF patients received corticosteroids (30% vs. 11%, p < 0.01) and vedolizumab (7% vs. 0.3%, p < 0.01) 30 days before surgery, but not anti-TNF agents (2% vs. 6%, p = 0.47). In addition, a higher proportion of CDIF patients had complicated surgeries, characterised as multiple procedures on the same day (91% vs. 44%, p < 0.01), post-operative stays longer than the 90th percentile (21 days) (48% vs. 22%, p < 0.01), or reoperation within 30 days (34% vs. 16%, p < 0.01) (Table 2). CDIF patients underwent a mean of 2.8 (SD 2.1) complicated surgeries during follow-up, compared with 0.5 (SD 1.1) for CD patients.
The rate of surgery over time in CDIF patients followed a different trend to CD patients (Fig. 3). In CDIF patients, CD-related abdominal surgeries initially decreased from 33 before 1980 to 17 surgeries per 100 patient-years in the 2000s, but subsequently increased to 30 surgeries per 100 patient-years after 2010. In CD patients, a consistent decline of CD-related abdominal surgeries was seen, from 17 surgeries per 100 patient-years before 1980 to four surgeries per 100 patient-years after 2010. These distinct trends were observed for both bowel resections and other abdominal surgeries.
Two factors contributed to the diverging trends between CDIF and CD patients. First, the median time-to-first-surgery increased from 2.86 (95% CI 2.27, 4.11) to 16.22 (14.94, 17.51) years in CD patients (p < 0.001) but did not significantly change in CDIF patients (p = 0.22). Second, there was a significant decrease in CD patients undergoing any bowel surgery during the follow-up period, from 75–14%, but there was no comparable decrease among CDIF patients.
Overall CD Activity
Ninety-two percent of CDIF (n = 155/168) and 62% of CD (n = 14,285/22,845) patients had severe CD activity in the year of CD diagnosis. During follow-up, the proportion experiencing severe activity decreased in both CDIF and CD patients, to 43% (n = 40/94) and 14% (n = 1,620/11,775) after 10 years, and 30% (n = 15/50) and 11% (n = 604/5,431) after 20 years, respectively (Fig. 4).
Overall, CDIF and CD patients had 50 and 19 years with severe CD activity per 100 patient-years, respectively (Table 2). For the first 10 years after CD diagnosis, 61% of CDIF patients (n = 103/168) had chronically severe disease and 6% (n = 10/168) had mild disease. In contrast, 15% of CD patients (n = 3,331/22,845) had chronically severe disease and 43% (n = 9,837/22,845) had mild disease (p < 0.01). Notably, on average, CDIF patients who were diagnosed with CD after 2000 experienced severe activity in eight out of the first 10 years, whereas patients with an earlier diagnosis experienced severe activity in six out of the first 10 years.
We observed no difference in disease activity patterns between CDIF patients who initiated, and those who did not initiate, biological therapy (Supplementary Results).
Working Capacity
During the follow-up period, 105 (66%) working-age CDIF patients had stopped work at least once, compared with 10,897 (58%) CD patients (p = 0.04). The employment activity rate was 60 per 100 eligible-working-years in CDIF patients, and 70 per 100 eligible-working-years in CD patients (p < 0.01).
Mortality
Seventy-seven (44%) CDIF and 5,182 (22.5%) CD patients died between 1973 and 2018. Compared with the age-, sex- and year-matched general population in Denmark, CDIF patients had a SMR of 3.66 (97.5% CI 2.79,4.72), while CD patients had a SMR of 1.66 (97.5% CI 1.61, 1.72). In both CDIF and CD patients, the excess mortality was higher in females, with a SMR of 4.71 (97.5% CI 3.32, 6.48) and 1.74 (97.5% CI 1.66, 1.81), respectively, and in patients with a young age of CD onset, who had a SMR of 7.66 (97.5% CI 1.68, 21.59) and 2.61 (97.5% CI 1.76, 3.71), respectively (Table 4).
Diseases of the digestive tract were attributed as the underlying cause of death in 51.9% of CDIF and 17.6% of CD patients. Excess deaths were observed in gastrointestinal cancers and haematological malignancies in CD, but not CDIF, patients (Supplementary Results).
When mortality was directly compared between CDIF and CD patients, the unadjusted all-cause mortality rate was 11.5%, 25% and 42.6% in CDIF patients at 10, 20 and 30 years after CD onset, and 15.2%, 27.1% and 39.3% in CD patients at 10, 20 and 30 years after CD onset, respectively (p = 0.94). However, after adjusting for age, sex, baseline comorbidities and CDIF patients surviving until IF onset, CDIF patients had hazard ratio of 3.42 (95% CI 2.55,4.59, p < 0.01) for mortality compared with CD patients (Supplementary Results).
{kind=link}