Based on the results of this study, it was possible to confirm the hypothesis that gluten- and casein-free dietary intervention seems to contribute to improving gut health and reducing possible hypersensitivity in individuals without a diagnosis of intolerance/allergies to these components. The sensitivity statement needs to be further investigated based on a more precise diagnosis [22], which was not the object of research in the present study. As for the hypothesis of changes in body mass and BMI, it was not possible to prove it. This result may be justified by the absence of a global energy reduction since there was no intervention or recommendation regarding the restriction of caloric intake from the habitual diet. However, this weight reduction can be found in long-term studies [23]. Although, adopting gluten-free diets has been linked to some nutritional deficiencies [24].
According to the Family Budget Survey (FBS), between 2008-2009 and 2017-2018, there was a reduction in the consumption of rice, beans, beef, bread, fruits, dairy products, processed meats, and sodas, but an increase in the consumption of sandwiches, signaling a worsening in the quality of the Brazilian diet [25]. In Brazil, the most consumed items, in order, are: cereals, milk, and fruits; Internationally, the three most consumed items are: cereals, vegetables, and milk. It can be said that the consumption patterns of both have some similarities, justified by globalization [26]. These data explain, in part, the high percentage of the presence of foods containing gluten and casein in the population's dietary habits [27,28], which may justify the dietary pattern of the public analyzed at the beginning of this research. This situation could be observed, in part, in students in the health sector at a public university in Recife, given the high consumption of simple carbohydrates, as well as other inadequacies that contributed to the association metabolic risk [29].
When mentioning hypersensitivity, in our findings, 19% of the volunteers in the EG group reported, through the applied questionnaire, being lactose intolerant, and another 24% reported having doubts about the possibility. However, when asked if they had undergone any type of test for confirmation and subsequent medical diagnosis of intolerance, only 9% of the entire sample in the EG had done so. Regarding gluten intolerance/allergy, the situation is the same as the previous one, 5% reported having it, and another 33% were unsure, but none of these reported a medical diagnosis of celiac disease or comproved hypersensibility. Thus without medical diagnosis, it can be inferred that a significant portion of the volunteers self-reported being intolerant, as well as suspected of "perceive hypersensitivity." This self-report is in line with the results conducted by other researchers, concluding that noticeable hesitation can be justified by the similarity between triggered symptoms [30].
This prevalence of sensitivity to gluten/wheat, for example, can be related to the technological process applied to the original wheat grain due to the loss of antioxidant compounds and the addition of inflammatory ingredients [31]. Regarding casein sensitivity, this may be associated with the possibility of the presence of β-casomorphin-7 (BCM-7), resulting from the hydrolysis of the A1 genetic variant of β-casein, which reflects intestinal discomfort and pro-inflammatory effects [32]. These reports may justify the symptomatic perception of these compounds, gluten, and casein.
In the EG group, it was observed that there was a predominance of females, as well as a strong adherence to GCFD. Adherence to nutritional recommendations was identified from the results obtained through the application of the FFQ and their respective significance at the end of the study when compared intra- and inter-groups. However, even without a diagnosis of celiac disease or casein/lactose allergy, the effect of dietary intervention in the EG on the MSQ and intestinal changes by the Bristol Scale was evident. Although reports indicate that following a restrictive diet in this regard appears to be difficult to adhere to, taking as an example the gluten-restricted diet, which appears to have greater adherence in celiac patients [33]. However, there is controversy regarding adherence even in celiac patients, which may have persistent symptomatology as a mediator [34].
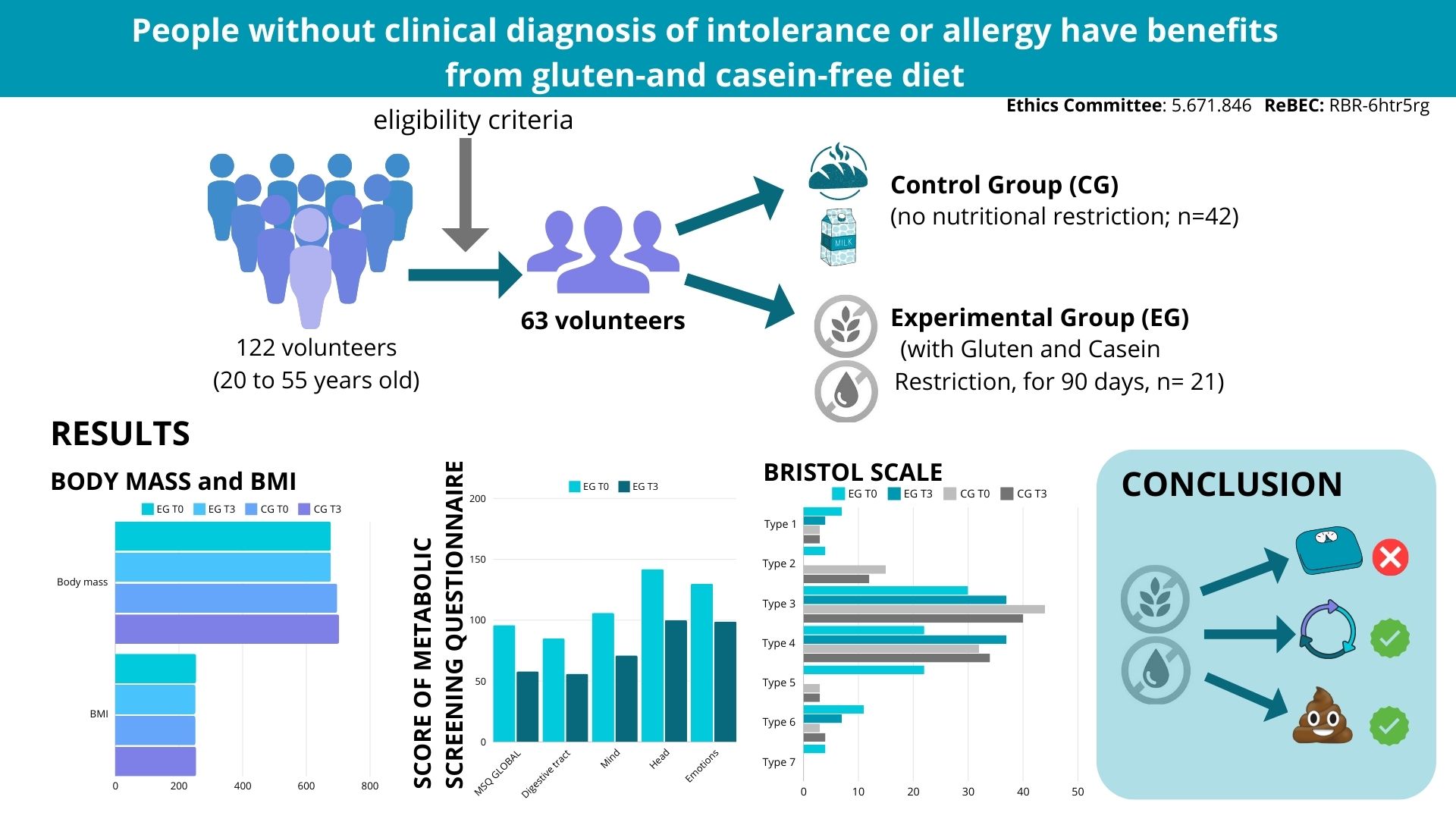
Furthermore, in this study, significant improvements were observed in symptomatological levels after GCFD, with a reduction in scores in the overall MSQ and in the domains of the digestive tract, mind, head, emotions, and nose. This can be explained by there being more than 50 toxic epitopes described in the gluten molecule related to cytotoxic, immunomodulatory activities and capable of altering intestinal permeability [35]. Regarding casein, there are also correlates of its contribution to immune response, intestinal permeability, and inflammation [6,7]. In addition, it is hypothesized that the A1 protein portion of β-casein is more inflammatory and detrimental to intestinal health when compared to the A2 protein portion of β-casein [36].
It is worth noting that the higher the representation of the score for the global classification of the MSQ, the greater the suspicion of hypersensitivity. Similarly, the greater the risk of developing intestinal dysbiosis and, consequently, the greater the influence of intestinal microbiota on the immune and neuroendocrine systems [12,37]. Through the findings of this study, it is verified that our intervention group initially presented similar characteristics, with a hypothesis of hypersensitivity and a risk of intestinal dysbiosis, which after GCFD resulted in a lower probability.
Results in the Bristol Scale also could be observed after the intervention period by demonstrating an improvement in stool consistency, as this instrument can indicate or be associated with a higher prevalence of food hypersensitivity due to changes in stool consistency and the presence of symptoms related to dysbiosis [38,39,40]. Although there was no statistical difference of the Bristol Scale in EG, the qualitative analysis clearly shows a reduction after intervention. Since there was an increase of 7% for Type 3 and 12% for Type 4. What corroborates with the intestinal result, as improvements in the digestive tract domain were also detected by the MSQ after the GCFD (gluten and casein free restriction). Therefore, the absence of gluten and casein in the usual diet appears to improve intestinal health.
Similarly, a gluten-free diet has shown possible therapeutic potential due to its contribution to changing the microbiota profile and modulating intestinal permeability [2,16]. This can be explained by gluten contributing to the intestinal inflammatory process by triggering immune, cellular, and humoral responses with consequent alteration in intestinal permeability [41,42]. Although the study did not evaluate inflammatory markers or microbiota profile, it is conjectured that the diet promoted an intestinal change with repercussions on intestinal health and the body as a whole.
In addition, it is evident that casein may be associated with abnormal intestinal permeability due to the possibility of incomplete absorption of peptides, which can trigger an inflammatory process [43,44,45]. The set of findings above suggest that there is a relationship between emotional and gastrointestinal symptoms, and, in the presence of intestinal dysbiosis can be assessed through the MSQ and Bristol Scale [46,47]. These associations may be related to the results for the following MSQ domains: mind, head, and emotions. However, these considerations still require further evidence regarding GCFD.
Based on the obtained results, it was possible to verify that the intervention with GCFD does not interfere with body mass and BMI. This finding reinforces the premise that the restriction of these compounds is not necessarily a strategy for reducing body weight, at least in the short term. This result is in agreement with the findings of another study that, after a gluten-free diet intervention in non-celiac, eutrophic women for three weeks, did not achieve significant reduction in body mass [48]. These results contradict studies that report an association between the exclusion of these components, gluten, and casein, with effectiveness in the weight loss process, as well as adherence to them. Excluding gluten from the diet may have beneficial effects on weight reduction, adiposity, insulin resistance, and inflammation [49]. It is important to mention that there is not enough evidence to support or dismiss the idea of inducing weight loss in healthy individuals [50]. However, the follow-up time may be a factor to be considered. Regarding cow's milk, which contains casein, when consumed in large quantities, it can trigger a process of metabolic inflammation and, thus, seem to hinder the weight loss process [51].
On the other hand, in the celiac population, for example, results related to BMI are observed [52]. Despite this, it is worth noting that there are currently no studies in the literature investigating GCFD in people without a diagnosis of allergy/intolerance to these components, preventing us from comparing our findings, especially considering it is a university population. In addition, it remains unknown, and its impact may differ in the presence of allergy. Furthermore, obese individuals also characterize an imbalanced microbiota [14,53], which makes them more vulnerable to the presence of signs and symptoms characteristic of intestinal dysbiosis associated with food hypersensitivity [10]. However, it is important to highlight the sample size and intervention time, which may not be sufficient, as limitations of the present study.
Interestingly, based on the results obtained, at the beginning of the study, 52% of the EG self-reported being infected with SARS-CoV-2, while responding to the questionnaire, and another 14% did not know how to respond. We cannot affirm, but there are intriguing doubts about possible metabolic impacts related, as well as possible health consequences; equally, it is not known how relevant this information is. However, it remains undefined and difficult to identify which inflammatory or hemodynamic changes are secondary to infection [54,55].
From the consulted literature, this study is pioneering in the designed research plan aimed at analyzing the impact of gluten and casein restriction on the gastrointestinal tract, applied to the academic community. Our results may stimulate other experimental designs and further investigations. We recognize the limitations of the study, such as the sample size of the EG; in addition, we did not assess biochemical measures to investigate and associate various inflammatory markers or of diagnostic or hypersensibility and compare them with the CG before and after the intervention. A possible bias in our study is that our sample was voluntary without double-bind. That is, these individuals previously suspected some dysfunction and chose to participate in the proposed intervention.
Other limitations are associated with unknown if the results observed in this study were due to: i) the combined removal of gluten and casein; ii) which potentially inflammatory compound presented itself more influentially individually, gluten or casein?; iii) or if foods containing these compounds in addition to these (gluten and casein). These foods still have other compounds that may intervene in combination in the final result, such as a high content of fats and simple carbohydrates, which requires further clarification in future research.
{kind=link}