Liver cancer commonly develops in hepatocytes and is called hepatocellular carcinoma (also known as primary liver cancer). As advances have been made in precision medicine, including oncology, improvements in clinical outcomes are expected [65]. Currently, a growing number of HCC patients are receiving cellular immunotherapy, indicating that HCC treatment has entered the era of immunotherapy. However, the complexity of patient conditions leads to an insufficient therapeutic response, drug resistance, and relapse during treatment. Currently, gene signatures, a type of biological function pattern created from the expression data of numerous genes, can be used to predict the prognosis and progression of several types of cancers [66, 67]. Here we constructed the AARGs signature associated with anoikis and autophagy and used the signature to predict the prognosis, disease progression, and therapy effectiveness in patients with HCC. The survival of HCC patients was accurately predicted using our signature.
Thirteen AARGs with differential expression were identified in this study, three of which were employed to create the AARGs signature using LASSO and Cox regression analyses. HCC patients could be classified into low- and high-risk groups with this signature. The ICGC, an independent validation cohort, confirmed the performance of this signature and demonstrated robust HCC survival prediction accuracy. Interestingly, in both the TCGA and ICGC cohorts, patients in the high-risk category exhibited lower tumour differentiation, progressed TNM stages, shorter survival durations, and higher fatality rates. HCC involves intricate mechanisms that are affected by a variety of variables, not simply AARGs, that aid in tumourigenesis. Consequently, we thought that additional important genes should be included in future signatures. Then we conducted the subgroup analyses and determined that the model could predict prognosis with precision, independent of individual clinical factor variations. In addition, model performance was validated in the TCGA and ICGC cohorts. The AARGs signature was found to be a significant independent prognostic factor. ROC analysis was performed to assess patient outcomes associated with time. In TCGA cohort, compared to long-term survival (4-year OS, AUC = 0.647), this model was fairly accurate at forecasting short-term survival (1-year OS, AUC = 0.734). Overall, the AARGs signature we developed in this study was demonstrated to be superior to the other prognostic signatures. To provide these patients with appropriate therapeutic strategies, such as using immunotherapy and changing the follow-up rate of individuals with high scores to track their performance, we can also use this sign to distinguish patients who have poor prognoses due to late-stage carcinoma stage at the time of clinical presentation.
It has previously been demonstrated that three genes [baculoviral IAP repeat containing 5 (BIRC5), mitogen-activated protein kinase 3 (MAPK3), and BRI1-associated kinase 1 (BAK1] ) in this signature are linked to the development of cancer. Jin et al. revealed a positive correlation exists between BIRC5 (survivalin) expression and NF-B expression in HCC tissues. It has been reported that both of these biomarkers are associated with poor prognoses in patients with HCC. Therefore, BIRC5 may be used as a biomarker to predict the prognosis of patients with HCC based on their biological characteristics [68]. Deng et al. revealed that MAPK1/3 regulates the degradation of ULK1 via the E3 ligase BTRC-mediated proteasomal degradation of its Lys48-linked ubiquitination, which contributes to the deregulation of ULK1 in breast cancer [69]. Xian et al. demonstrated that MIEF1 loss also results in mitochondrial depolarisation mediated by BAK1. As a consequence of pro-apoptotic effectors BAX and BAK1, MIEF1 plays a critical role in mitochondrial-dependent apoptosis [70]. In the present study, we combined these three genes to construct a prognostic signature. Further investigations are required to determine the prognostic value of these three AARGs in HCC and their underlying mechanisms.
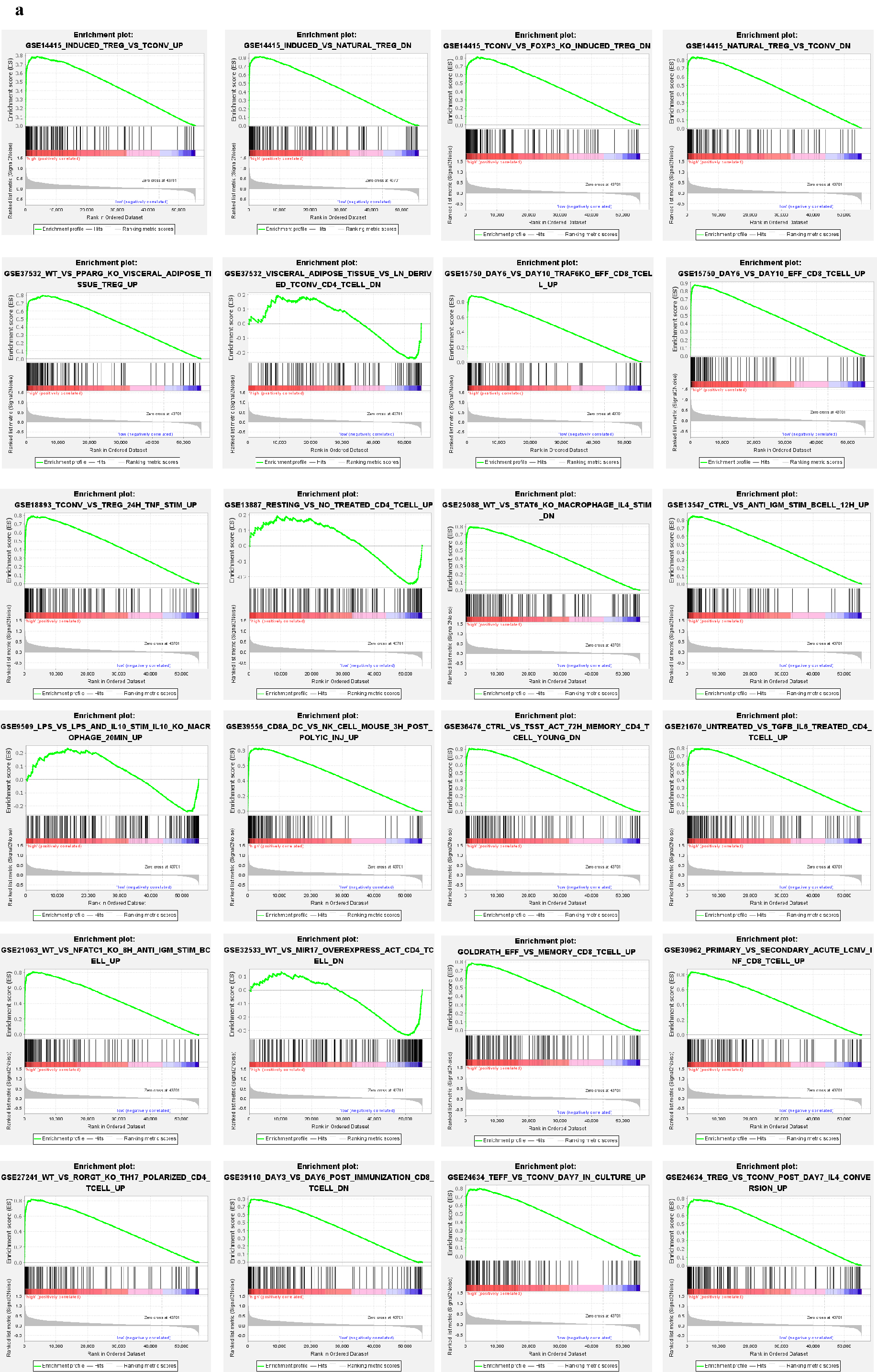
Current research suggests that the tumour microenvironment (TME) is a setting that promotes the survival and growth of tumour cells [71]. The TME is composed of infiltrating stromal cells, immune cells, tumour cells, cytokines, and stromal microenvironments [72] and plays an essential role in tumour proliferation, angiogenesis, invasion, and metastasis. Consequently, more detailed information on the TME can lead to potential therapies to benefit patients with advanced HCC [73]. In the present study, we divided patients into high- and low-risk groups based on their signatures. According to our findings, patients with high-risk scores had superior immune responses than those in the low-risk group because they had more infiltrating Macrophages M0, T cell follicular helper cells, and T cell regulatory cells. Immunotherapy, especially ICB, has resulted in a paradigm shift in HCC treatment [74]. There was a substantial difference between the two patient groups receiving effective care when the immune checkpoint genes (CD274, CTLA4, HAVCR2, LAG3, PDCD1, and TIGHT) were stratified by risk score. However, in this signature, high-risk patients have poor treatment options for ICB therapy. We conducted GSEA for these two groups of patients to evaluate their immune status. This result is similar to the above results. We performed drug sensitivity analysis of our signature using the IC50 which can identify the sensitivity of chemotherapeutic and small-molecule drugs. The responses to various chemotherapeutic treatments (etoposide, foretinib, gefitinib, gemcitabine) varied significantly between the high- and low-risk groups. In our analysis, low-risk patients had an increased monocyte count, T cell CD4 + memory, and naive B cell count, which confirms previous reports of immunological profiles in HCC cases [75–77], such profiles are indicative of of negative prognosis. in these patients. The high-risk groups show aggressive tumour growth caused by stemness [78] and CTLA4 [79]. Overall, these findings are consistent with our findings.
There are currently a few published prognostic models based on AnRGs [17] or AuRGs [23]. Anoikis or autophagy alone does not provide good accuracy or sensitivity for prognosis because of the diversity of HCC and the complexity of its microenvironment. In our study, we first combined AnRGs and AuRGs to construct an AARGs signature that is robust in predicting the prognosis and progression of HCC. By establishing a nomogram, the AARGs signature could be easily used in clinical settings. We conducted an immune analysis of our signature to provide individualised treatment options for patients with HCC. However, this study was limited by the following factors: 1) There is always some bias in retrospective studies, which is why additional verification of this signature through multicentre datasets is warranted; 2) To better understand these three AARGs, comprehensive functional studies are required to shed light on the detailed mechanisms. The next stage of our research will involve analysing the interaction mechanisms and clinical and bioinformatics data.
{kind=link}