The findings of this study highlight polypharmacy, defined as the concurrent use of five or more medications, as a significant contributor to postoperative morbidity and mortality among older adults with hip fractures. The prevalence of polypharmacy in the study sample was notably high, and there was a clear and robust association between the severity of polypharmacy and an increased incidence of both major and total complications during hospitalization. Furthermore, patients with polypharmacy exhibited elevated mortality rates across short-, medium-, and long-term follow-ups.
These results underscore the critical importance of meticulous medication management in this vulnerable patient population to enhance clinical outcomes. They are consistent with numerous studies in the scientific literature that have similarly demonstrated the detrimental impact of polypharmacy on health outcomes in older adults [11, 12, 16, 17, 23, 29].
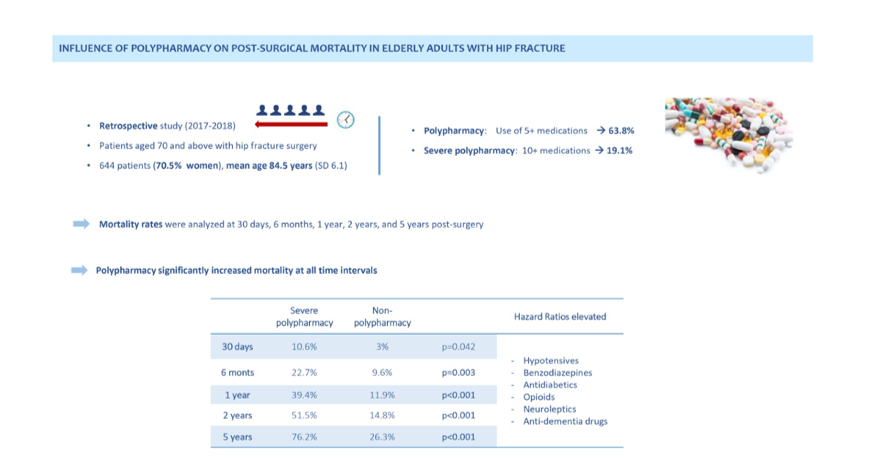
The impact of polypharmacy on clinical outcomes has been extensively studied and documented [30–33], demonstrating effects that extend beyond immediate postoperative risks to encompass long-term health complications [34]. In our study sample, the prevalence of global polypharmacy was 63.8%, with a clear correlation observed between the severity of polypharmacy and increases in both Charlson Comorbidity Index (CCI) scores and the incidence of major and total complications during hospitalization.
Furthermore, existing research has highlighted the heightened likelihood and risk of neck of femur fractures associated with polypharmacy, along with its link to elevated postoperative mortality rates [20, 35]. These findings underscore the critical need for comprehensive management strategies to mitigate the adverse effects of polypharmacy in older adults, particularly those undergoing surgical interventions for hip fractures.
These findings underscore the complexity of managing patients with polypharmacy and emphasize the necessity for vigilant monitoring to prevent and promptly address associated complications [16, 18, 19]. These complications may encompass requirements for red blood cell transfusions, falls, infections, and cardiovascular events, all contributing to heightened morbidity and prolonged recovery periods.
Interestingly, our study did not find a significant difference in the length of hospital stay, suggesting that the severity of complications, rather than the duration of hospitalization, may be a critical factor influenced by polypharmacy. This underscores the potential role of specialized care from geriatricians within orthogeriatric units in attenuating the impact of hospital admission duration on patient outcomes.
In this context, this study underscores the crucial role of comprehensive geriatric assessment (CGA) in managing elderly patients with hip fractures. CGA facilitates early identification of frailty, comorbidities, and specific patient needs [6, 9]. By implementing CGA, healthcare providers can optimize pharmacological treatment, thereby reducing the burden of polypharmacy and enhancing clinical outcomes.
CGA involves a thorough evaluation of medical, functional, psychological, and social factors, enabling the development of personalized care plans that address all aspects of a patient's health. Effective coordination between geriatricians and other specialists is essential for managing polypharmacy and mitigating its associated complications [18, 36]. This approach ensures comprehensive care tailored to the unique needs of elderly patients with hip fractures, ultimately improving their overall health outcomes.
The analysis reveals that patients with polypharmacy exhibit elevated mortality rates at 30 days, 6 months, 1 year, 2 years, and 5 years post-surgery compared to those without polypharmacy. Specifically, severe polypharmacy (≥ 10 drugs) was associated with an even greater increase in mortality. These findings align with previous studies indicating that the use of multiple medications increases the risk of death in geriatric patients [5, 21, 25].
The relationship between the number of medications and mortality may be explained by the higher probability of adverse drug interactions, the increased complexity and burden of comorbidities, and heightened frailty due to cumulative drug side effects [17]. These factors underscore the critical importance of meticulously managing polypharmacy in elderly patients, emphasizing the necessity for strategies that mitigate these risks and enhance overall patient outcomes.
The study underscores the impact of hypotensive drugs, benzodiazepines/hypnotics, antidiabetics, opioids, neuroleptics, and anti-dementia drugs on five-year mortality. While these medications are beneficial for specific conditions, they pose a high-risk profile in geriatric patients due to their side effects and potential to exacerbate frailty [13, 20].
Managing these medications in older patients should be prioritized, emphasizing deprescription strategies and regular review of medication regimens to mitigate risks [11, 12]. This approach necessitates a multidisciplinary effort involving primary care physicians, pharmacists, and specialists to ensure that each patient's medication plan is optimized for safety and efficacy. Comprehensive medication management is essential, advocating for regular reviews and deprescribing protocols in orthogeriatric units. Tools like STOPP/START criteria or Beers Criteria can help identify inappropriate medications.
Deprescribing should be approached cautiously, involving patients and caregivers in the decision-making process. Educating them about the risks of polypharmacy and the benefits of reducing medication can enhance adherence to deprescribing plans and improve satisfaction with care. Patient-centered deprescribing interventions have been shown to effectively reduce medication use and improve health outcomes [12].
A multidisciplinary team approach involving geriatricians, pharmacists, primary care physicians, and surgeons is crucial to consider all health aspects in medication decisions. Regular interdisciplinary case conferences can enhance patient outcomes through collaborative management [14].
There are no differences in comorbidity estimated by the CCI, although the results may be confounded by the higher prevalence of ischemic heart disease, heart failure, stroke, chronic kidney failure, and diabetes.
It is essential to acknowledge several limitations of this study. Firstly, its retrospective design introduces the potential for bias in data collection. Furthermore, while this study can establish associations, it cannot determine causality. Despite controlling for variables such as age, sex, and comorbidities, there remains a possibility that unconsidered factors may have influenced the observed results. Additionally, although the loss rate was relatively low at 7%, it could potentially impact the study's findings. In addition, no potential adverse effects of the prescribed medication at home were recorded. The number of modified START/STOPP criteria and the number of medications discontinued at discharge were not collected.
Moving forward, future prospective and multicentre studies are warranted to validate these findings assess specific deprescribing interventions on clinical outcomes. Incorporating comprehensive geriatric assessments (CGA) into routine care for elderly hip fracture patients is essential for identifying frailty and comorbidities, leading to individualized care plans that optimize treatment and reduce polypharmacy [10]. Additionally, leveraging health information technology can help monitor polypharmacy and prevent adverse drug events through real-time alerts for healthcare providers. Future research should focus on integrating these technological tools in geriatric care settings.
{kind=link}