Our retrospective record review revealed that the COVID-19 pandemic resulted in a large drop in travel clinic volumes and associated revenue from the Pre-COVID period and that these decreases were still present in the Late COVID-19 period although increases were occurring. This corresponds to the large decrease in international travel numbers due to travel restrictions and concerns about contracting COVID. Although our volume of inpatient Infectious Diseases consultation requests increased dramatically throughout both COVID periods, the corresponding drop in our travel and outpatient patient volumes created the effect of only minimal revenue increases, if any, despite the added time efforts noted by our providers (S1, S2). This loss in practice revenue owing to loss of Travel Clinic volumes had not yet recovered to the pre-pandemic levels by the end of Late COVID.
The drop in pre-travel consultation numbers and revenue seen in our clinic were also seen in other travel clinics in the US and in other countries. An International Society of Travel Medicine (ISTM) survey performed in April and May of 2021, revealed that 70% of respondents reported substantial reductions in travel clinic volumes.15 A report on the impact in Southern Europe showed an overall drop of 75–90% for pre-travel assessments.16 Such reductions in travel clinic volumes could have a devastating impact on free-standing travel clinics or sites that cannot easily shift personnel and resources elsewhere.17 This could result in a reduction in public health benefits that travel medicine services can provide. Also impacting the revenue decline would be the loss in income attributable to fewer vaccinations administered during COVID.
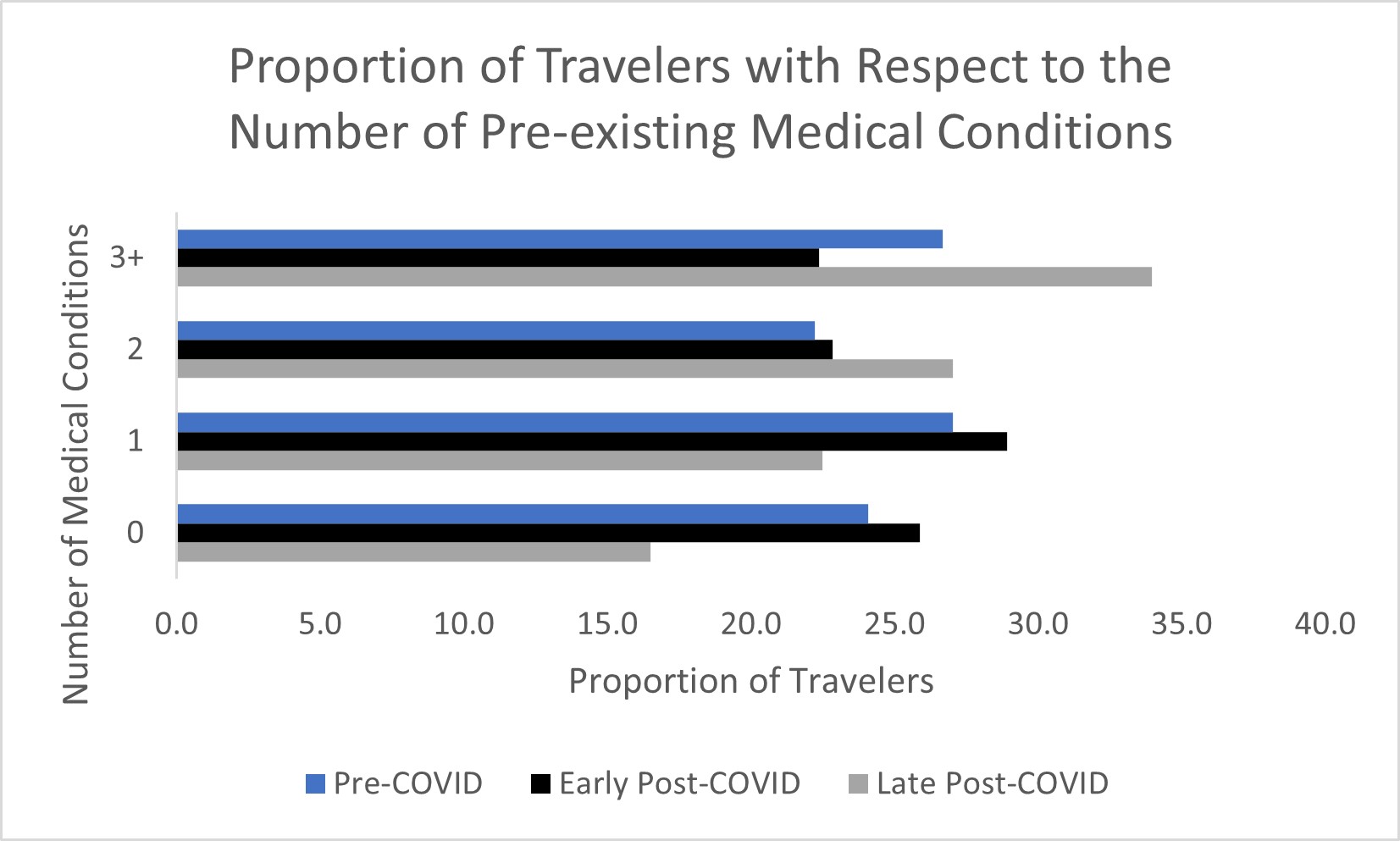
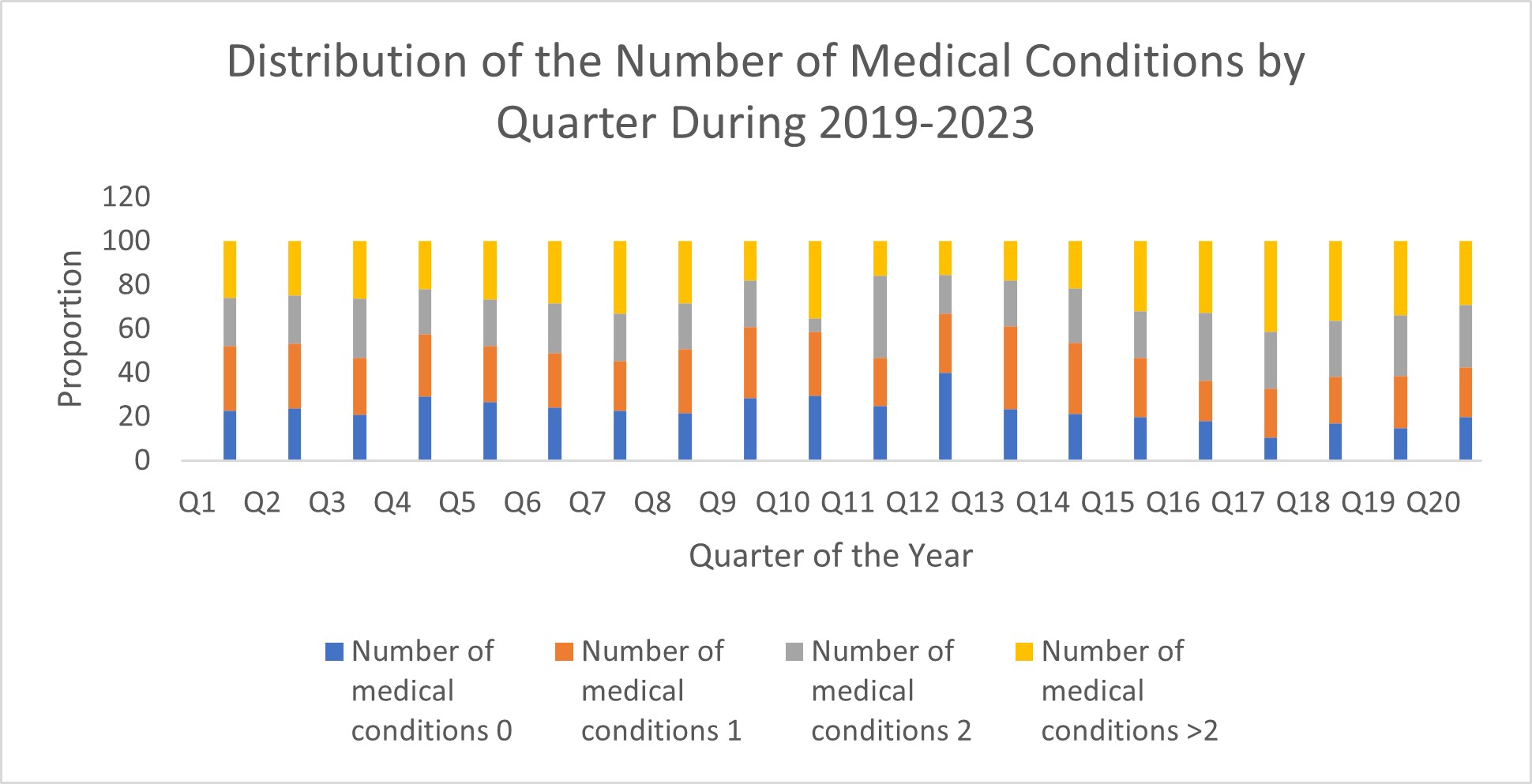
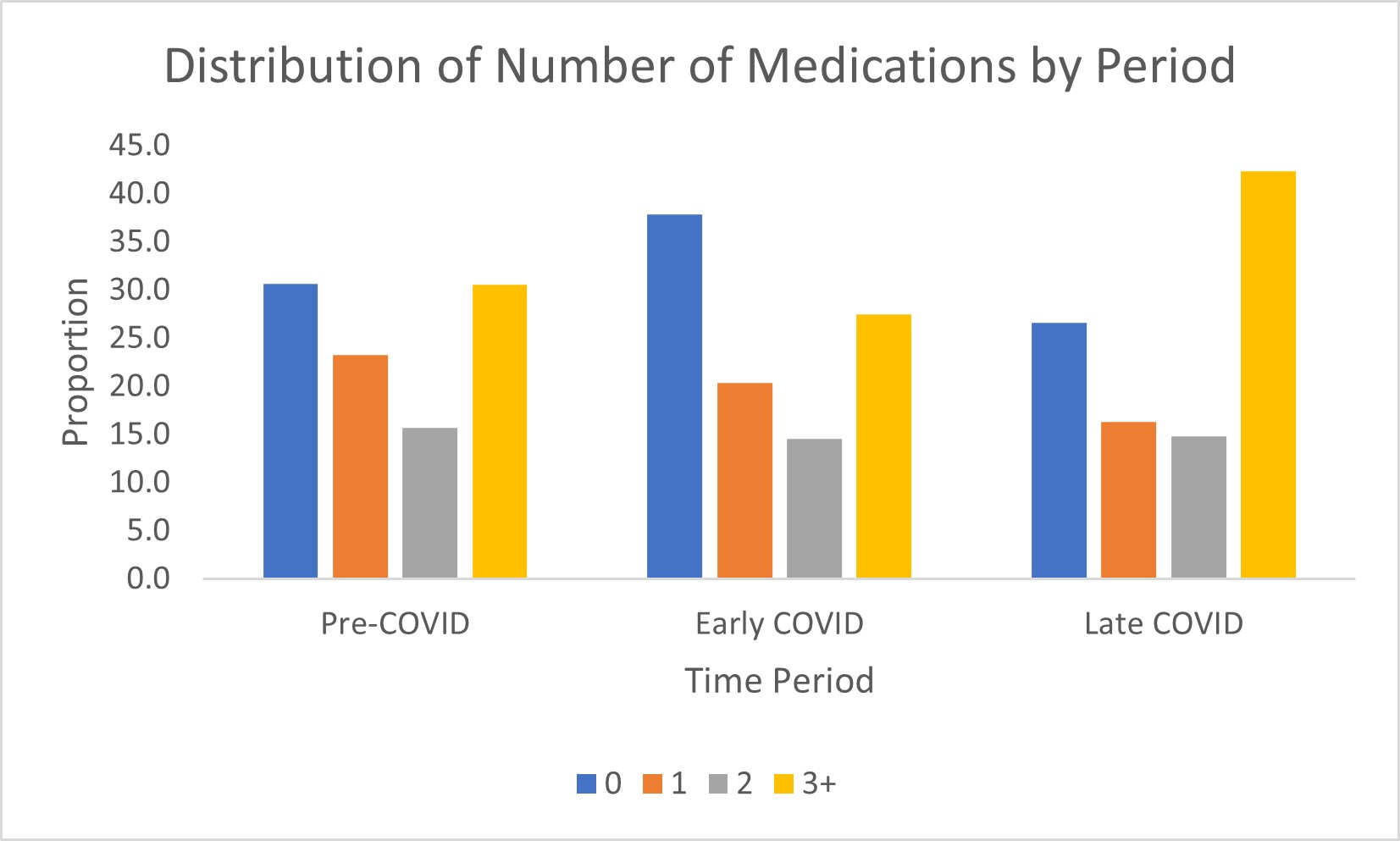
Traveler demographics themselves changed significantly, with younger travelers consulting pre-travel services more during the Early-COVID-19 period and overall, the travelers were healthier, when looking at the number of pre-existing medical conditions and the number of current medications. Interestingly, most of these demographic features were recalibrating back toward baseline during the Late-COVID-19 period, particularly a much higher proportion of senior travelers and corresponding shorter trip durations.
VFR travel proportionally rose dramatically during Early COVID-19, while travel for leisure and business decreased significantly. In addition to an increase in VFR travel, we also noted a significant surge in the proportion of travelers leaving for humanitarian work. Most of the changes in reason for travel seem to re-calibrate quickly in the Late COVID period.
We also found a significant increase in proportional travel to Africa, especially by VFR travelers, and especially for longer durations. This may reflect individuals traveling back to countries of origin during pandemic, perhaps either for family or financial reasons. The proportional increase of travelers to Africa may in part reflect the desire or need to obtain yellow fever vaccination to assist country entry. VFR travel has been a main driver in more recent returns to higher international travel volume with some forecasts suggesting a 17% compounded annual growth rate from 2021 − 25.18 This trend is likely to continue.
Along with the improved health of travelers noted in the Early COVID-19 period, there were fewer vaccines given to patients during this period and throughout the Late COVID-19 period. It was not clear if the reduction in vaccines administered during Early/Late COVID-19, reflected increased declination or provider assessment of vaccine need. Perhaps some of the reduction in vaccination we saw during Early COVID-19 may have been in part due to a significant increase in the proportion of self-pay travelers (not insured) who may have opted to forgo some of the recommended immunizations due to cost concerns. Alternatively, considering the corresponding increase in VFR travel, fewer vaccines were ordered. It is well documented that VFR travelers are often under-vaccinated for similar destinations as other travelers and more often may decline recommended vaccinations.19 Certain vaccinations did show high acceptance rates during the Early COVID-19, including Yellow Fever, hepatitis A, and typhoid vaccines.
Consistent with other data, travel durations were longer with more travelers going for over 4 weeks. The destinations changed significantly as well with more trips to the African continent and correspondingly fewer trips to South America and Southeast Asia. We believe that destination changes were a result of global travel restrictions as well as destinations to which VFR travelers returned.18,19,20 It is possible that many VFR travelers decided to isolate themselves and work remotely for their jobs, from their countries of origin and to be with family members, in association, perhaps with a lower cost of living.
The changes in our traveler demographics were similar to a prior analysis of the larger GTEN database, reviewing over 18,000 consultations which showed significant differences among international travelers during COVID-19, with longer durations of travel, an increase in proportions of younger travelers and an increase in VFR travel.6 Travel to Africa increased significantly in this larger study, with a reduction in travel to Asia, similar to our findings. That review included a large pediatric population, showing a 263% relative increase through the COVID-19 period. It is likely that this was a consistent theme across the US, particularly during early COVID-19.
We believe our data is helpful for future planning for pandemics or during global travel restrictions. Our 85% drop in travel-revenue through Early COVID-19 was substantial and can add to the stress of an already overburdened Infectious Diseases or other medical practice. Practices that rely heavily on Travel Medicine as part of their revenue stream will need to consider having remediation plans in place to weather future restrictions should they occur. Furthermore, addressing the particular needs of younger, particularly VFR travelers, would be important going forward, realizing that many do not seek pre-travel consultation and may be at higher risk for preventable adverse outcomes including, malaria typhoid fever, and hepatitis.21
There are a few limitations to our analysis:
Data collected by the GTEN are limited to travelers who seek pre-travel advice from a GTEN site and hence these results cannot be generalized to a broader pre-travel population, many of whom might not seek pre-travel consultation and have been shown to differ from GTEN travelers.9
Second, in the GTEN, the travelers self-report their medical conditions, medications, and reason for travel. This can be corrected at the pre-travel visit by the provider onsite, but there is the potential for travelers to omit or overstate the number of potential health problems as compared with a detailed provider history. As such, the traveler’s overall health cannot always be accurately gauged by the results of the pre-travel survey.
Lastly, this study was from a single site within a specific type of healthcare network. Our findings may not be generalizable to other travel clinics or to the healthcare networks that support them.
{kind=link}
{kind=link}
{kind=link}